Biomechanics/Movements
Unit Outline
Learning Objectives
At the end of this unit, you should be able to:
- Describe how muscles attach to bones to produce movement.
- Describe the principle of muscular antagonism in movement, using the forearm as an example.
- Define the following terms: lever, fulcrum, resistance, effort.
- Describe three types of levers and give an example of each type in the human body.
- Explain the biomechanical principles and functioning of a lever system.
- Specify four factors that determine the type of movement accomplished by a muscle.
- Specify some of the criteria used in the naming of muscles.
- Describe, using specific examples, 16 types of movements characteristic of skeletal muscle contractions.
Part 1: Skeletal Muscle Anatomy
Muscle Attachment to the Skeleton
To move the skeleton, the tension created by the contraction of the fibers in most skeletal muscles is transferred to the tendons. The tendons are strong bands of dense, regular connective tissue that connect muscles to bones. The bone connection is why this muscle tissue is called skeletal muscle.
To pull on a bone, that is, to change the angle at its synovial joint, which essentially moves the skeleton, a skeletal muscle must be attached to a fixed part of the skeleton. The moveable end of the muscle that attaches to the bone being pulled is called the muscle’s insertion, whereas the end of the muscle attached to a fixed (stabilized) bone is called the origin.
Muscular Antagonism
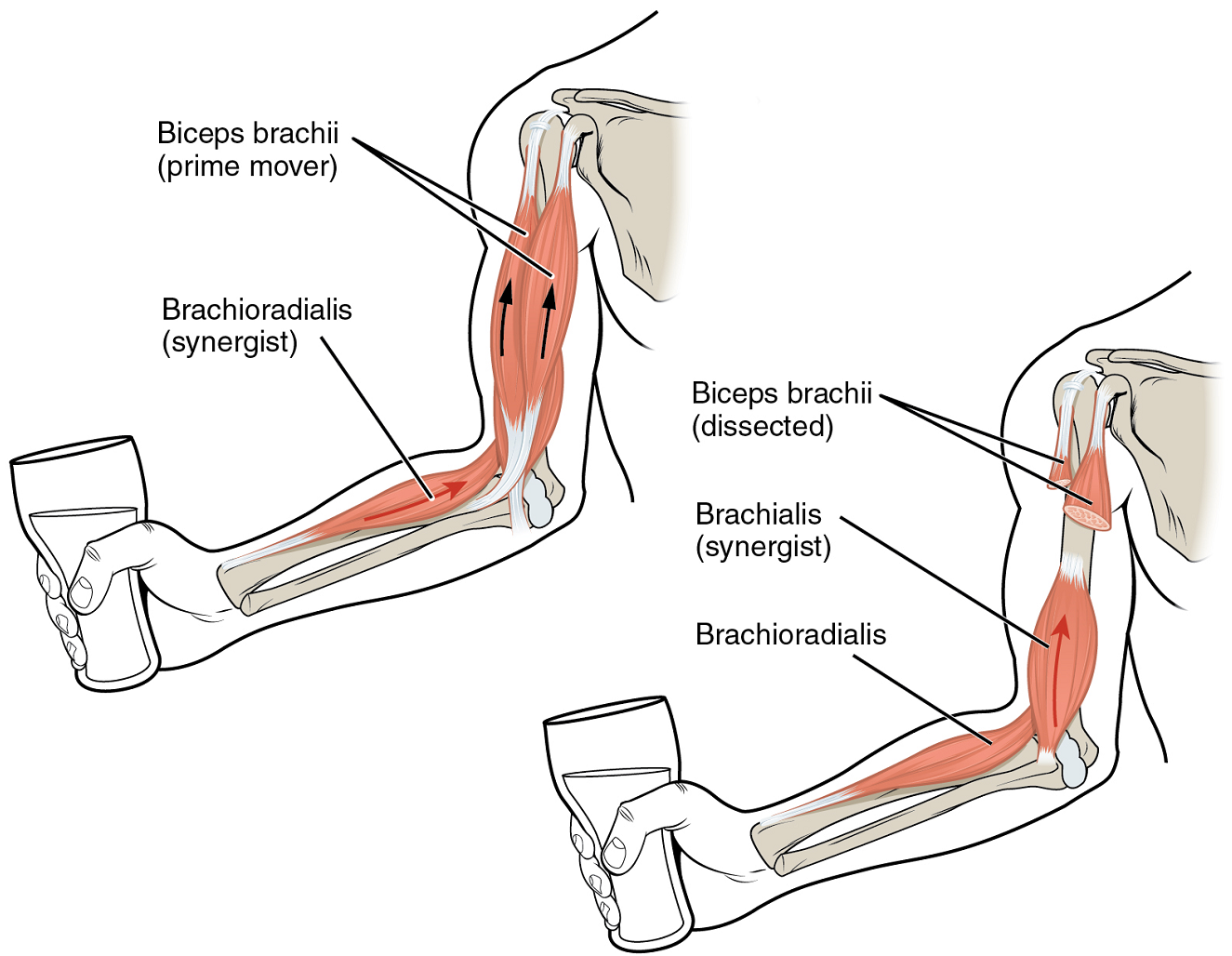
Although a number of muscles may be involved in an action, the principal muscle involved is called the prime mover, or agonist. To lift a cup, a muscle called the biceps brachii is the prime mover; however, because this muscle can be assisted by the brachialis, the brachialis is called a synergist in this action (Figure 12.1). A synergist can also be a fixator, which stabilizes the bone that is the attachment for the prime mover’s origin.
A muscle with the opposite action of the prime mover is called an antagonist. Antagonists play two important roles in muscle function: (1) they maintain body or limb position, such as holding the arm out or standing erect, and (2) they control rapid movement, as in shadowboxing without landing a punch, and thereby check the motion of a limb.
For example, to extend the knee, a group of four muscles called the quadriceps femoris in the anterior compartment of the thigh is activated. These muscles would be called the agonists of knee extension. However, to flex the knee, an opposite or antagonistic set of muscles called the hamstrings is activated. Flexing the knee involves the hamstrings muscles as the agonists and the quadriceps femoris muscles as the antagonists. As you can see, the terms agonist and antagonist are associated with a particular movement, and these terms can be reversed for opposing movements. See Table 12.1 for a list of some common agonists and antagonists.
| Agonist | Antagonist | Movement |
|---|---|---|
| Biceps brachii (in anterior compartment of arm) | Triceps brachii (in posterior compartment of arm) | The biceps brachii flexes the forearm, whereas the triceps brachii extends it |
| Hamstrings (group of three muscles in the posterior compartment of thigh) | Quadriceps femoris (group of four muscles in anterior compartment of thigh) | The hamstrings flex the leg, whereas the quadriceps femoris extend it |
| Flexor digitorum superficialis and flexor digitorum profundus (in anterior compartment of forearm) | Extensor digitorum (in posterior compartment of forearm) | The flexor digitorum superficialis & profundus flex the fingers and hand at the wrist, whereas the extensor digitorum extends the fingers and hand at the wrist |
Muscles Without Attachments to the Skeleton
Some skeletal muscles do not pull on the skeleton to cause movements. For example, the muscles that produce facial expressions have their insertions and origins in the skin, and particular muscles contract to form a smile or frown, form sounds or words, or raise the eyebrows. There are also such skeletal muscles in the tongue, as well as in the external urinary and anal sphincters that allow for voluntary regulation of urination and defecation, respectively. Another example is the diaphragm, which contracts and relaxes to change the volume of the pleural cavities without moving the skeleton.
Test Your Knowledge
Describe Skeletal Muscle Anatomy
- Describe muscle attachment to the skeleton.
- Define muscular antagonism.
Part 2: Lever Systems
Skeletal muscles do not work by themselves. Muscles are arranged in pairs based on their functions. For muscles attached to the bones of the skeleton, the connection determines the force, speed, and range of movement. These characteristics depend on one another and can explain the general organization of the muscular and skeletal systems.
General Characteristics
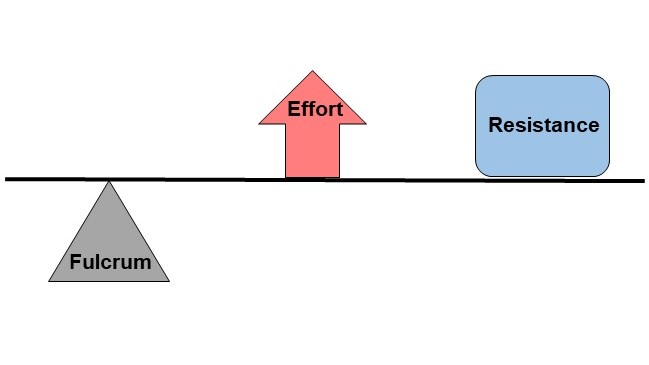
The skeleton and muscles act together, as a lever, to move the body. Have you ever used the back of a hammer to remove a nail from wood? The handle acts as a lever and the head of the hammer acts as a fulcrum, the fixed point that the force is applied to when you pull back or push down on the handle. The effort applied to this system is the pulling or pushing on the handle to remove the nail, which is the resistance to the movement of the handle in the system. The resistance is also sometimes called the load. Our musculoskeletal system works in a similar manner, with bones being stiff levers and the articular endings of the bones—encased in synovial joints—acting as fulcrums. The resistance would be an object or body part being moved, or any resistance to a movement (e.g. your head when you are lifting it). The effort, or applied force, comes from contracting particular skeletal muscles.
The characteristics and operation of a particular lever system are mainly determined by distances and forces. The two opposing forces are the effort and resistance. There are two main distances to consider: (1) the effort arm, which is the distance from the fulcrum to the insertion point of the skeletal muscle delivering most of the effort, and (2) the resistance arm, which is the distance between the fulcrum and the bulk of the resistance.
In order for movement to occur (e.g. when lifting a weight in your hand), the effort produced by one or several muscles needs to overcome the resistance. When the lever system is balanced, the two opposing forces applied at their respective distances from the fulcrum work to maintain a body posture or carry a particular weight without moving it. Thus, in a balanced lever system, the effort times the effort arm is equal to the resistance times the resistance arm. This is the basic formula used to calculate relationships between forces and distances in a lever system:
Effort x Effort arm = Resistance x Resistance arm
Lever systems that can move heavy loads over short distances using little effort are referred to as “power levers”. Conversely, lever systems that can quickly move light loads over large distances using a large amount of effort are referred to as “speed levers”. The location of the insertion point of a muscle (or muscles) delivering the effort relative to the resistance determines whether a lever system operates as a power lever or speed lever. For example, a lever system with a muscle insertion point close to the joint (fulcrum) and a resistance far away from the joint will move a particular object relatively fast over a large distance with a great range of motion. However, the muscle(s) involved need(s) to deliver a large effort for the movement to occur. Another lever system with a resistance close to the fulcrum which is supported by a muscle (or muscles) inserting far away from the fulcrum will require a small effort to support or move the resistance. However, the resistance will only be moved over a short distance and slowly.
There are several types of lever systems in the body, identified as either first-class, second-class or third-class levers.
First-class levers
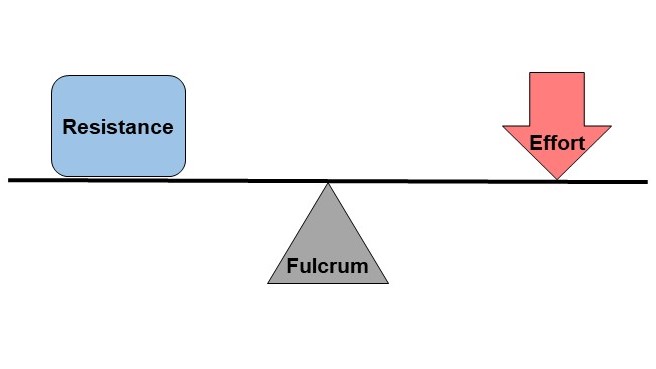
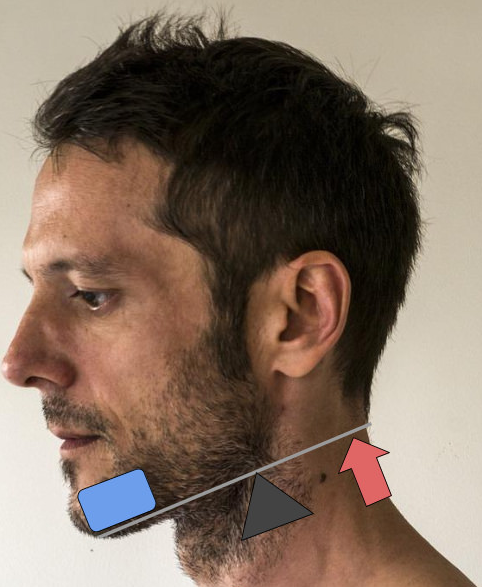
First-class levers are the simplest types of lever, where the two forces, the effort and the resistance, are applied on opposite sides of the fulcrum (Figure 12.2). In the body, the best example of a first-class lever is the way your head is raised off your chest (Figure 12.3). The posterior neck muscles produce the effort, the facial skeleton is the resistance, and the atlanto-occipital joint behaves as the fulcrum.
Second-Class Levers
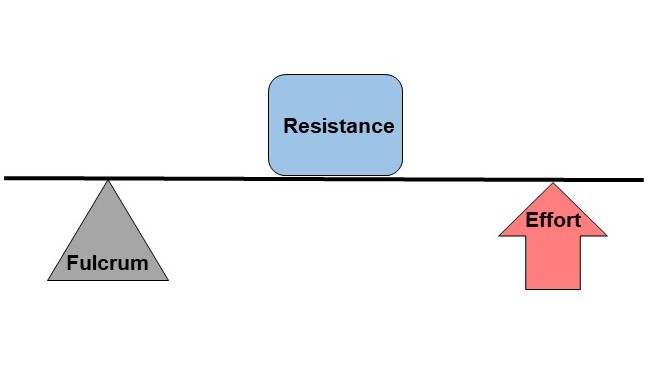
Second-class levers have the resistance between the effort and the fulcrum (Figure 12.4). The effort is closer to the resistance than the fulcrum, which allows a large resistance to be moved by a small amount of effort. However, this means that the resistance will be moved at a relatively slow pace and can only be moved a short distance. Any time you stand up on your toes, as shown in Figure 12.5, you are using a second-class lever. The weight of your body acts as the resistance, your calf muscles produce the effort, and the joints in the balls of your feet act as fulcrums.

Third-Class Levers
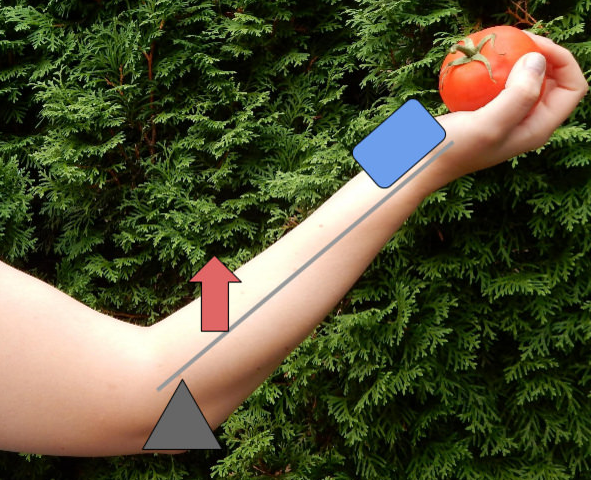
Third-class levers are the most common type of levers in your body (Figure 12.6). The effort is applied between the fulcrum and the resistance, which allows the resistance to be moved relatively quickly over large distances. When you lift your hand by flexing your biceps brachii, you are using a third-class lever. The elbow joint acts as the fulcrum, the biceps brachii produces the effort, and the weight of your hand is the resistance being lifted (Figure 12.7).
You can also watch the above video on Lever System: Biomechanics by clicking the link or scanning the QR code below.

Test Yourself
1. Define the following terms: lever, fulcrum, resistance, effort.
2. Write single-sentence definitions for each of these terms:
- Lever
- Fulcrum
- Resistance
- Effort
3. Describe three types of levers and give an example of each type in the human body.
4. Clearly indicate the following on each diagram from the chapter:
- The exact location where the resistance is applied to the lever
- The exact location where the effort is applied to the lever
- The resistance arm
- The effort arm
5. Explain the biomechanical principles and functioning of a lever system.
6. Using the flexion of the forearm as an example, explain how a lever system is used to move body parts or maintain the posture of body parts.
7. Then, report the following for the lever system described above:
- The length of the resistance arm, in cm
- The length of the effort arm, in cm
- The effort exerted by the biceps brachii, if the resistance is:
- 1 kg
- 10 kg
- 25 kg
- The effort exerted by the biceps brachii to lift a resistance of 10 kg, if the distance between the elbow joint and the insertion point of the biceps brachii remains the same (5 cm), but the total length of the forearm is:
- 25 cm
- 35 cm
- 50 cm
- The effort exerted by the biceps brachii to lift a resistance of 10 kg, if the total length of the forearm remains the same (35 cm) but the distance between the elbow joint and the insertion point of the biceps brachii is:
- 1 cm
- 5 cm
- 7 cm
- 28 cm
Part 3: Types of Body Movement
Synovial joints allow the body a tremendous range of movements. Each movement at a synovial joint results from the contraction or relaxation of the muscles that are attached to the bones on either side of the articulation. The type of movement that can be produced at a synovial joint is determined by four factors:
- Orientation of the muscle. Each muscle is attached at an origin and an insertion. The origin of the muscle is its attachment to the bone that will remain relatively stable when that muscle contracts. It is the bone to which the muscle is anchored. The other end of the muscle will be its insertion, which is its attachment to the bone which will move when that muscle contracts. The orientation of the muscle, which bone it is anchored to and which bone it inserts in, will determine the movement.
- Action of other muscles that may insert and/or originate on the same bone(s) that when any particular muscle contracts, the bone will be moved in a particular direction, different from the direction any single muscle may produce. It is not uncommon to see the same muscle being involved in two or more different movements.
- Type of joint between the bones. There are a number of different types of joints between bones. Only the synovial joint allows for any significant movement. Each specific joint is limited in the movement it can provide because of the shape of the ends of the bones in the joint and because of the tension in the ligaments holding the bones together.
- Muscle tension. This is a limitation that works in a similar manner to tension in the ligaments. An example of the role of muscle tension is demonstrated when touching one’s toes with the knees straight. The movement is restricted by the tension of the hamstring muscles.
While the ball-and-socket joint gives the greatest range of movement at an individual joint, in other regions of the body, several joints may work together to produce a particular movement. Overall, each type of synovial joint is necessary to provide the body with its great flexibility and mobility. There are many types of movement that can occur at synovial joints (Table 13.1). Movement types are generally paired, with one being the opposite of the other. Body movements are always described in relation to the anatomical position of the body: upright stance, with upper limbs to the side of body and palms facing forward.
| Type of Joint | Movement | Examples |
|---|---|---|
| Pivot | Uniaxial joint; allows rotational movement | Atlantoaxial joint (C1-C2 vertebrae articulation); proximal radioulnar joint |
| Hinge | Uniaxial joint; allows flexion/extension movements | Knee; elbow; ankle; interphalangeal joints of fingers and toes |
| Condyloid | Biaxial joint; allows flexion/extension, abduction/adduction, and circumduction movements | Metacarpophalangeal (knuckle) joints of fingers; radiocarpal joint of wrist; metatarsophalangeal joints of toes |
| Saddle | Biaxial joint; allows flexion/extension, abduction/adduction, and circumduction movements | First carpometacarpal joint (carpometacarpal joint of the thumb); sternoclavicular joint |
| Plane | Multiaxial joint; allows inversion/eversion of the foot, flexion/extension, and lateral flexion of the vertebral column | intertarsal joints of foot; superior-inferior articular process articulations between vertebrae |
| Ball-and-socket | Multiaxial joint; allows flexion/extension, abduction/adduction, circumduction, and medial/lateral rotation movements | Shoulder joint, hip joint |
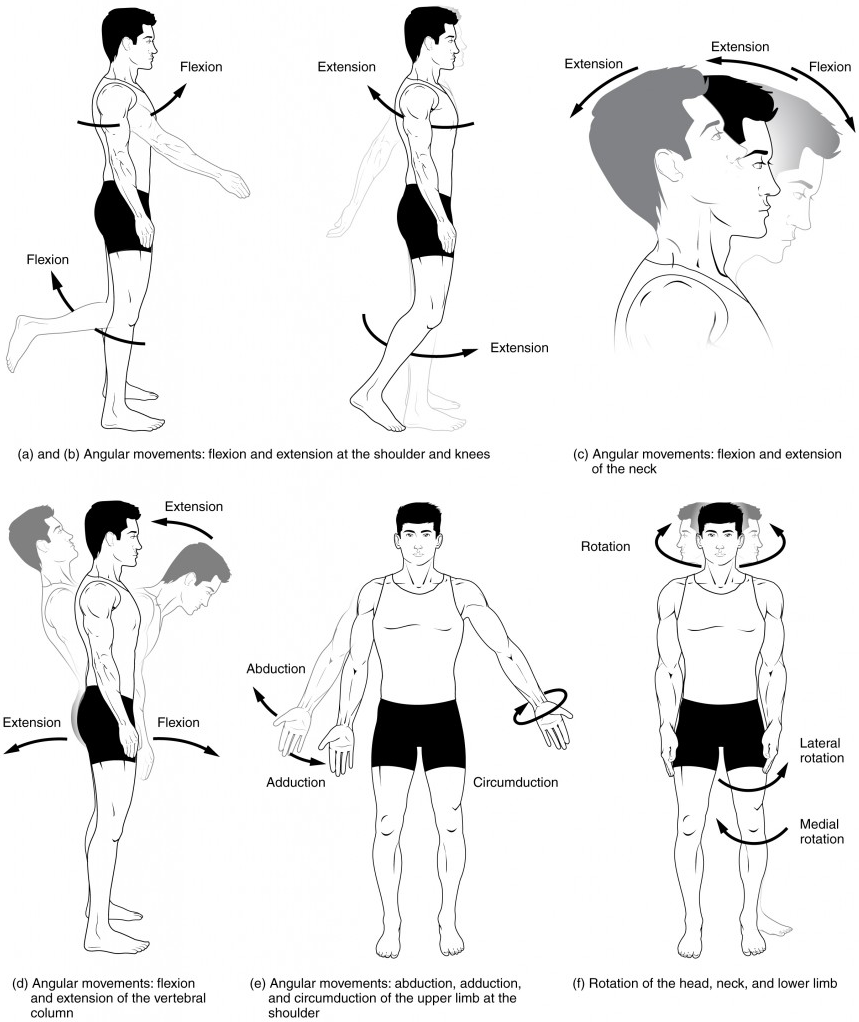
Flexion and Extension
Flexion and extension are movements that take place within the sagittal plane and involve anterior or posterior movements of the body or limbs. For the vertebral column, flexion is an anterior (forward) bending of the neck or body, while extension involves a posterior-directed motion, such as straightening from a flexed position or bending backward. Lateral flexion is the bending of the neck or body toward the right or left side. These movements of the vertebral column involve both the symphysis joint formed by each intervertebral disc, as well as the plane type of synovial joint formed between the inferior articular processes of one vertebra and the superior articular processes of the next lower vertebra.
In the limbs, flexion decreases the angle between the bones (bending of the joint), while extension increases the angle and straightens the joint. For the upper limb, all anterior-going motions are flexion, and all posterior-going motions are extension. These include anterior-posterior movements of the arm at the shoulder, the forearm at the elbow, the hand at the wrist, and the fingers at the metacarpophalangeal and interphalangeal joints. For the thumb, extension moves the thumb away from the palm of the hand, within the same plane as the palm, while flexion brings the thumb back against the index finger or into the palm. These motions take place at the first carpometacarpal joint. In the lower limb, bringing the thigh forward and upward is flexion at the hip joint, while any posterior-going motion of the thigh is extension. Note that extension of the thigh beyond the anatomical (standing) position is greatly limited by the ligaments that support the hip joint. Knee flexion is the bending of the knee to bring the foot toward the posterior thigh, and extension is the straightening of the knee. Flexion and extension movements are seen at the hinge, condyloid, saddle, and ball-and-socket joints of the limbs (Figure 13.5a–d).
Hyperextension
Hyperextension is the abnormal or excessive extension of a joint beyond its normal range of motion, thus resulting in injury. Similarly, hyperflexion is excessive flexion at a joint. Hyperextension injuries are common at hinge joints such as the knee or elbow. In cases of “whiplash” in which the head is suddenly moved backward and then forward, a patient may experience both hyperextension and hyperflexion of the cervical region.
Abduction and Adduction
Abduction and Adduction: Abduction and adduction motions occur within the coronal plane and involve medial-lateral motions of the limbs, fingers, toes, or thumb. Abduction moves the limb laterally away from the midline of the body, while adduction is the opposing movement that brings the limb toward the body or across the midline. For example, abduction is raising the arm at the shoulder joint, moving it laterally away from the body, while adduction brings the arm down to the side of the body. Similarly, abduction and adduction at the wrist moves the hand away from or toward the midline of the body. Spreading the fingers or toes apart is also abduction, while bringing the fingers or toes together is adduction. For the thumb, abduction is the anterior movement that brings the thumb to a 90° perpendicular position, pointing straight out from the palm. Adduction moves the thumb back to the anatomical position, next to the index finger. Abduction and adduction movements are seen at condyloid, saddle, and ball-and-socket joints (Figure 13.55e).
Circumduction
Circumduction is the movement of a body region in a circular manner, in which one end of the body region being moved stays relatively stationary, while the other end describes a circle. It involves the sequential combination of flexion, adduction, extension, and abduction at a joint. This type of motion is found at biaxial condyloid and saddle joints and at multiaxial ball-and-socket joints (Figure 13.5e).
Rotation
Rotation can occur within the vertebral column, at a pivot joint, or at a ball-and-socket joint. Rotation of the neck or body is the twisting movement produced by the summation of the small rotational movements available between adjacent vertebrae. At a pivot joint, one bone rotates in relation to another bone. This is a uniaxial joint, and thus rotation is the only motion allowed at a pivot joint. For example, at the atlantoaxial joint, the first cervical (C1) vertebra (atlas) rotates around the dens, the upward projection from the second cervical (C2) vertebra (axis). This allows the head to rotate from side to side as when shaking the head “no.” The proximal radioulnar joint is a pivot joint formed by the head of the radius and its articulation with the ulna. This joint allows for the radius to rotate along its length during pronation and supination movements of the forearm.
Rotation can also occur at the ball-and-socket joints of the shoulder and hip. Here, the humerus and femur rotate around their long axis, which moves the anterior surface of the arm or thigh either toward or away from the midline of the body. Movement that brings the anterior surface of the limb toward the midline of the body is called medial (internal) rotation. Conversely, rotation of the limb so that the anterior surface moves away from the midline is lateral (external) rotation (Figure 13.5f). Be sure to distinguish medial and lateral rotation, which can only occur at the multiaxial shoulder and hip joints, from circumduction, which can occur at either biaxial or multiaxial joints.
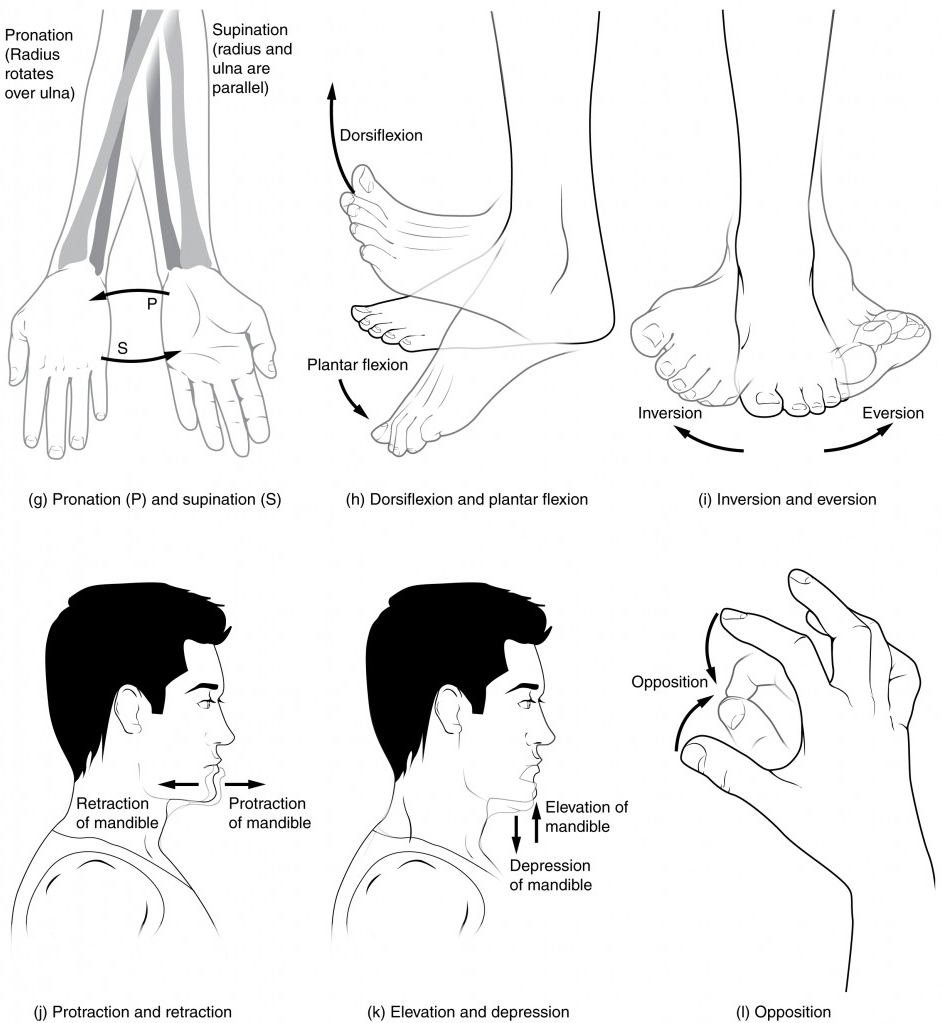
Supination and Pronation
Supination and pronation are movements of the forearm. In the anatomical position, the upper limb is held next to the body with the palm facing forward. This is the supinated position of the forearm. In this position, the radius and ulna are parallel to each other. When the palm of the hand faces backward, the forearm is in the pronated position, and the radius and ulna form an X-shape.
Supination and pronation are the movements of the forearm that go between these two positions. Pronation is the motion that moves the forearm from the supinated (anatomical) position to the pronated (palm backward) position. This motion is produced by the rotation of the radius at the proximal radioulnar joint, accompanied by movement of the radius at the distal radioulnar joint. The proximal radioulnar joint is a pivot joint that allows for the rotation of the head of the radius. Because of the slight curvature of the shaft of the radius, this rotation causes the distal end of the radius to cross over the distal ulna at the distal radioulnar joint. This crossing over brings the radius and ulna into an X-shape position. Supination is the opposite motion, in which rotation of the radius returns the bones to their parallel positions and moves the palm to the anterior facing (supinated) position. It helps to remember that supination is the motion you use when scooping up soup with a spoon (Figure 13.6g).
Dorsiflexion and Plantar Flexion
Dorsiflexion and plantar flexion are movements at the ankle joint, which is a hinge joint. Lifting the front of the foot, so that the top of the foot moves toward the anterior leg is dorsiflexion, while lifting the heel of the foot from the ground or pointing the toes downward is plantar flexion. These are the only movements available at the ankle joint (Figure 13.6h).
Inversion and Eversion
Inversion and eversion are complex movements that involve the multiple plane joints among the tarsal bones of the posterior foot (intertarsal joints) and thus are not motions that take place at the ankle joint. Inversion is the turning of the foot to angle the bottom of the foot toward the midline, while eversion turns the bottom of the foot away from the midline. The foot has a greater range of inversion than eversion motion. These are important motions that help to stabilize the foot when walking or running on an uneven surface and aid in the quick side-to-side changes in direction used during active sports such as basketball, racquetball, or soccer (Figure 13.6i).
Protraction and Retraction
Protraction and retraction are anterior-posterior movements of the scapula or mandible. Protraction of the scapula occurs when the shoulder is moved forward, as when pushing against something or throwing a ball. Retraction is the opposite motion, with the scapula being pulled posteriorly and medially toward the vertebral column. For the mandible, protraction occurs when the lower jaw is pushed forward, to stick out the chin, while retraction pulls the lower jaw backward (Figure 13.6j).
Depression and Elevation
Depression and elevation are downward and upward movements of the scapula or mandible. The upward movement of the scapula and shoulder is elevation, while a downward movement is depression. These movements are used to shrug your shoulders. Similarly, elevation of the mandible is the upward movement of the lower jaw used to close the mouth or bite on something, and depression is the downward movement that produces the opening of the mouth (Figure 13.6k).
Test Your Knowledge
- Specify four factors which determine the type of movement accomplished by a muscle.
- Define “origin” and “insertion” as these terms pertain to skeletal muscles.
- Describe how the locations of the origin(s) and insertion(s) of a skeletal muscle affect the movement produced when that muscle contracts.
- Describe one specific example of a skeletal muscle that participates in multiple different movements, and then explain how it is possible for a skeletal muscle to participate in multiple different movements.
- Describe how the movement produced by contraction of a skeletal muscle is influenced by the structure of a joint about which the muscle moves the bone on which it inserts.
- Describe how tension in ligaments, tendons, and skeletal muscles can limit the range of motion available when a skeletal muscle contracts.
- Describe, using specific examples, 16 types of movements characteristic of skeletal muscle contractions.
- Clearly define each of the following terms.
- Flexion
- Extension
- Rotation
- Circumduction
- Abduction
- Adduction
- Elevation
- Depression
- Protraction
- Retraction
- Eversion
- Inversion
- Plantar flexion
- Dorsiflexion
- Pronation
- Supination
- Clearly describe (including an example of the body part being moved) and distinguish between each of the following pairs of terms:
- Flexion and extension
- Adduction and abduction
- Eversion and inversion
- Protraction and retraction
- Rotation and circumduction
- Plantar flexion and dorsiflexion
- Elevation and depression
- Pronation and supination
Test Your Knowledge
1. Define the following terms: lever, fulcrum, resistance, effort.
2. Write single-sentence definitions for each of these terms:
- Lever
- Fulcrum
- Resistance
- Effort
3. Describe three types of levers and give an example of each type in the human body.
4. Clearly indicate the following on each diagram from the chapter:
- The exact location where the resistance is applied to the lever
- The exact location where the effort is applied to the lever
- The resistance arm
- The effort arm
5. Explain the biomechanical principles and functioning of a lever system.
6. Using the flexion of the forearm as an example, explain how a lever system is used to move body parts or maintain the posture of body parts.
7. Then, report the following for the lever system described above:
- The length of the resistance arm, in cm
- The length of the effort arm, in cm
- The effort exerted by the biceps brachii, if the resistance is:
- 1 kg
- 10 kg
- 25 kg
- The effort exerted by the biceps brachii to lift a resistance of 10 kg, if the distance between the elbow joint and the insertion point of the biceps brachii remains the same (5 cm), but the total length of the forearm is:
- 25 cm
- 35 cm
- 50 cm
- The effort exerted by the biceps brachii to lift a resistance of 10 kg, if the total length of the forearm remains the same (35 cm) but the distance between the elbow joint and the insertion point of the biceps brachii is:
- 1 cm
- 5 cm
- 7 cm
- 28 cm
Practice
For the following question, drag each of the answers at the bottom of the box into the correct answer space.
Image Descriptions Figure 12.1 image description: The brachioradialis, in the forearm, and brachialis, located deep to the biceps brachii in the upper arm, are both synergists that aid in this motion. [Return to image.]
General anatomical term for a hole or opening (usually in bone. Plural = foramina).
Neck
Middle layer of the meninges named for the spider-web–like trabeculae that extend between it and the pia mater.
Lower back, below the ribs.
Neck
General anatomical term for a hole or opening (usually in bone. Plural = foramina).
Region of the adult brain that retains its name from embryonic development and includes the thalamus and hypothalamus.
Change in the membrane potential that varies in size, depending on the size of the stimulus that elicits it.
Lower back, below the ribs.
Mid-back, where ribs attach to vertebrae.
The space between the visceral and parietal pleurae.
Back of the knee.
Mid-back, where ribs attach to vertebrae.
Gray matter region of the spinal cord in which sensory input arrives, sometimes referred to as the dorsal horn.
Gray matter region of the spinal cord in which sensory input arrives, sometimes referred to as the dorsal horn.
Gray matter of the spinal cord containing multipolar motor neurons, sometimes referred to as the ventral horn.
Gray matter of the spinal cord containing multipolar motor neurons, sometimes referred to as the ventral horn.
Region of the spinal cord gray matter in the thoracic, upper lumbar, and sacral regions that is the central component of the sympathetic division of the autonomic nervous system.
Region of the spinal cord gray matter in the thoracic, upper lumbar, and sacral regions that is the central component of the sympathetic division of the autonomic nervous system.
Branch of the autonomic nervous system associated with emergency systems (“fight or flight”).
Branch of the autonomic nervous system associated with emergency systems (“fight or flight”).
Region of the sacrum, bone forming the back part of the pelvic cavity.
Two-headed muscle that crosses the shoulder and elbow joints to flex the forearm while assisting in supinating it and flexing the arm at the shoulder.
Major region of the diencephalon that is responsible for relaying information between the cerebrum and the hindbrain, spinal cord, and periphery.
Thumb
Half of the midbrain tectum that is part of the brain stem auditory pathway.
The portion of the ventricular system that is in the region of the brain stem and opens into the subarachnoid space through the median and lateral apertures.
The portion of the ventricular system that is in the region of the brain stem and opens into the subarachnoid space through the median and lateral apertures.
Two-dimensional, vertical plane that divides the body or organ into right and left sides.
Middle region of the adult brain that develops from the mesencephalon.
Functional division of the nervous system that is responsible for homeostatic reflexes that coordinate control of cardiac and smooth muscle, as well as glandular tissue.
Connection of the ventricular system between the third and fourth ventricles located in the midbrain.
Describes a position below or lower than another part of the body proper; near or toward the tail (in humans, the coccyx, or lowest part of the spinal column); also referred to as caudal.
Describes a position above or higher than another part of the body proper; also referred to as cranial.
Space between the arachnoid mater and pia mater that contains CSF and the fibrous connections of the arachnoid trabeculae.
Diffuse region of gray matter throughout the brain stem that regulates sleep, wakefulness, and states of consciousness.
Half of the midbrain tectum that is part of the brain stem auditory pathway.
Glial cell type that filters blood at the choroid plexus.
Tough, fibrous, outer layer of the meninges that is attached to the inner surface of the cranium and vertebral column and surrounds the entire CNS.
Outpocket of the arachnoid membrane into the dural sinuses that allows for reabsorption of CSF into the blood.
Half of the midbrain tectum that is responsible for aligning visual, auditory, and somatosensory spatial perceptions.
Nucleus within the basal nuclei that is part of the indirect pathway.
Outpocket of the arachnoid membrane into the dural sinuses that allows for reabsorption of CSF into the blood.
Lowest (most inferior) part of the brain, controlling many autonomic functions including heart rate, breathing, and digestion.
Connection of the ventricular system between the third and fourth ventricles located in the midbrain.
Swelling at the end of an axon where neurotransmitter molecules are released onto a target cell across a synapse.
Shape of a neuron that has multiple processes—the axon and two or more dendrites.
Swelling at the end of an axon where neurotransmitter molecules are released onto a target cell across a synapse.
See parasagittal plane
See frontal plane
See parasagittal plane
Thigh bone; the single bone of the thigh.
Any of the venous structures surrounding the brain, enclosed within the dura mater, which drain blood from the CNS to the common venous return of the jugular veins.
Any of the venous structures surrounding the brain, enclosed within the dura mater, which drain blood from the CNS to the common venous return of the jugular veins.
Circuit of a reflex that involves a sensory input and motor output, or an afferent branch and an efferent branch, and an integrating center to connect the two branches.
One of a pair of major veins located in the neck region that flows parallel to the common carotid artery that is more or less its counterpart; primarily drains blood from the brain, receives the superficial facial vein, and empties into the subclavian vein.
One of a pair of major veins located in the neck region that flows parallel to the common carotid artery that is more or less its counterpart; primarily drains blood from the brain, receives the superficial facial vein, and empties into the subclavian vein.
Sensory ganglion attached to the posterior nerve root of a spinal nerve.
Sensory ganglion attached to the posterior nerve root of a spinal nerve.
One of twelve nerves connected to the brain that are responsible for sensory or motor functions of the head and neck.
One of twelve nerves connected to the brain that are responsible for sensory or motor functions of the head and neck.
Tenth cranial nerve; responsible for the autonomic control of organs in the thoracic and upper abdominal cavities.
Central abdominopelvic region including the belly button.
(In nervous system) a localized collection of neuron cell bodies that are functionally related; a “center” of neural function (plural= nuclei).
Tenth cranial nerve; responsible for the autonomic control of organs in the thoracic and upper abdominal cavities.
Circuit of a reflex that involves a sensory input and motor output, or an afferent branch and an efferent branch, and an integrating center to connect the two branches.
