
The social construction of health is a major research topic within medical sociology. At first glance, the concept of a social construction of health does not seem to make sense. After all, if the disease is a measurable, physiological problem, then there can be no question of socially constructing disease, right? Well, it’s not that simple. The idea of the social construction of health emphasizes the socio-cultural aspects of the discipline’s approach to physical, objectively definable phenomena. Sociologists Conrad and Barker (2010) offer a comprehensive framework for understanding the major findings of the last fifty years of development in this concept. Their summary categorizes the findings in the field under three subheadings: the cultural meaning of illness, the social construction of the illness experience, and the social construction of medical knowledge.
The Cultural Meaning of Illness
Many medical sociologists contend that illnesses have both a biological and an experiential component, and that these components exist independently of each other. Our culture, not our biology, dictates which illnesses are stigmatized and which are not, which are considered disabilities and which are not, and which are deemed contestable (meaning some medical professionals may find the existence of this ailment questionable) as opposed to definitive (illnesses that are unquestionably recognized in the medical profession) (Conrad and Barker 2010).
For instance, sociologist Erving Goffman (1963) described how social stigmas hinder individuals from fully integrating into society. In essence, Goffman (1963) suggests we might view illness as a stigma that can push others to view the ill in an undesirable manner. The stigmatization of illness often has the greatest effect on the patient and the kind of care he or she receives. Many contend that our society and even our healthcare institutions discriminate against certain diseases—like mental disorders, AIDS, venereal diseases, and skin disorders (Sartorius 2007). Facilities for these diseases may be sub-par; they may be segregated from other healthcare areas or relegated to a poorer environment. The stigma may keep people from seeking help for their illness, making it worse than it needs to be.
Contested illnesses are those that are questioned or questionable by some medical professionals. Disorders like fibromyalgia or chronic fatigue syndrome may be either true illnesses or only in the patients’ heads, depending on the opinion of the medical professional. This dynamic can affect how a patient seeks treatment and what kind of treatment he or she receives.
The Social Construction of the Illness Experience
The idea of the social construction of the illness experience is based on the concept of reality as a social construction. In other words, there is no objective reality; there are only our own perceptions of it. The social construction of the illness experience deals with such issues as the way some patients control the manner in which they reveal their diseases and the lifestyle adaptations patients develop to cope with their illnesses.
In terms of constructing the illness experience, culture and individual personality both play a significant role. For some people, a long-term illness can have the effect of making their world smaller, more defined by the illness than anything else. For others, illness can be a chance for discovery, for re-imaging a new self (Conrad and Barker 2007). Culture plays a huge role in how an individual experiences illness. Widespread diseases like AIDS or breast cancer have specific cultural markers that have changed over the years and that govern how individuals—and society—view them.
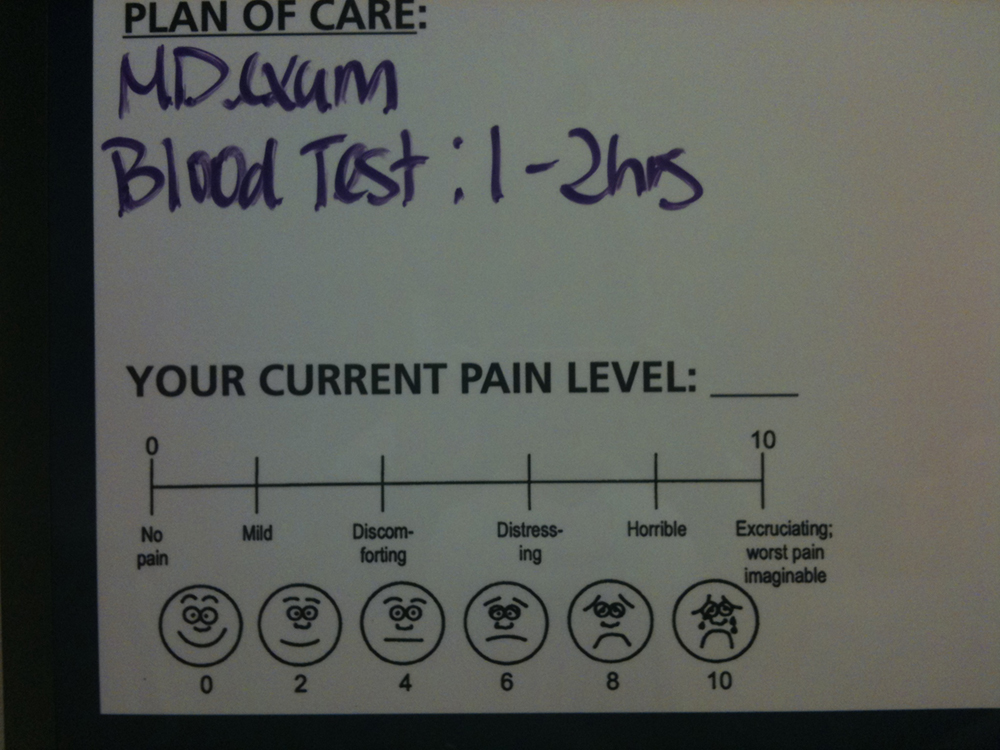
Today, many institutions of wellness acknowledge the degree to which individual perceptions shape the nature of health and illness. Regarding physical activity, for instance, the Centers for Disease Control (CDC) recommends that individuals use a standard level of exertion to assess their physical activity. This Rating of Perceived Exertion (RPE) gives a more complete view of an individual’s actual exertion level, since heartrate or pulse measurements may be affected by medication or other issues (Centers for Disease Control 2011a). Similarly, many medical professionals use a comparable scale for perceived pain to help determine pain management strategies.
The Social Construction of Medical Knowledge
Conrad and Barker show how medical knowledge is socially constructed; that is, it can both reflect and reproduce inequalities in gender, class, race, and ethnicity. Conrad and Barker (2011) use the example of the social construction of women’s health and how medical knowledge has changed significantly over the course of a few generations. For instance, in the early nineteenth century, pregnant women were discouraged from driving or dancing for fear of harming the unborn child, much as they are discouraged, with more valid reason, from smoking or drinking alcohol today.
SOCIAL POLICY AND DEBATE
Has Breast Cancer Awareness Gone Too Far?

Every October, the world turns pink. Football and baseball players wear pink accessories. Skyscrapers and large public buildings are lit with pink lights at night. Shoppers can choose from a huge array of pink products. In 2014, people wanting to support the fight against breast cancer could purchase any of the following pink products: KitchenAid mixers, Master Lock padlocks and bike chains, Wilson tennis rackets, Fiat cars, and Smith & Wesson handguns. You read that correctly. The goal of all these pink products is to raise awareness and money for breast cancer. However, the relentless creep of pink has many people wondering if the pink marketing juggernaut has gone too far.
Pink has been associated with breast cancer since 1991 when the Susan G. Komen Foundation handed out pink ribbons at its 1991 Race for the Cure event. Since then, the pink ribbon has appeared on countless products, and then by extension, the color pink has come to represent support for a cure for the disease. No one can argue about the Susan G. Komen Foundation’s mission—to find a cure for breast cancer—or the fact that the group has raised millions of dollars for research and care. However, some people question if, or how much, all these products really help in the fight against breast cancer (Begos 2011).
The advocacy group Breast Cancer Action (BCA) positions itself as a watchdog of other agencies fighting breast cancer. They accept no funding from entities, like those in the pharmaceutical industry, with potential profit connections to this health industry. They’ve developed a trademarked “Think Before You Pink” campaign to provoke consumer questioning of the end contributions made to breast cancer by companies hawking pink wares. They do not advise against “pink” purchases; they just want consumers to be informed about how much money is involved, where it comes from, and where it will go. For instance, what percentage of each purchase goes to breast cancer causes? BCA does not judge how much is enough, but it informs customers and then encourages them to consider whether they feel the amount is enough (Think Before You Pink 2012).
BCA also suggests that consumers make sure that the product they are buying does not actually contribute to breast cancer, a phenomenon they call “pinkwashing.” This issue made national headlines in 2010 when the Susan G. Komen Foundation partnered with Kentucky Fried Chicken (KFC) on a promotion called “Buckets for the Cure.” For every bucket of grilled or regular fried chicken, KFC would donate fifty cents to the Komen Foundation, with the goal of reaching 8 million dollars: the largest single donation received by the foundation. However, some critics saw the partnership as an unholy alliance. Higher body fat and eating fatty foods have been linked to increased cancer risks, and detractors, including BCA, called the Komen Foundation out on this apparent contradiction of goals. Komen’s response was that the program did a great deal to raise awareness in low-income communities, where Komen previously had little outreach (Hutchison 2010).
What do you think? Are fundraising and awareness important enough to trump issues of health? What other examples of “pinkwashing” can you think of?
13.2 Global Health
Learning Objectives
- Define social epidemiology
- Apply theories of social epidemiology to an understanding of global health issues
- Understand the differences between high-income and low-income nations
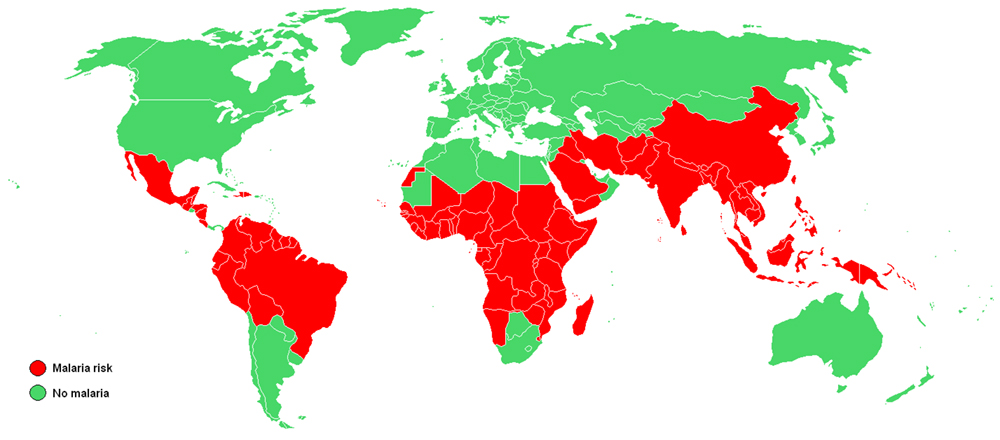
Social epidemiology is the study of the causes and distribution of diseases. Social epidemiology can reveal how social problems are connected to the health of different populations. These epidemiological studies show that the health problems of high-income nations differ greatly from those of low-income nations. Some diseases, like cancer, are universal. But others, like obesity, heart disease, respiratory disease, and diabetes, are much more common in high-income countries and are a direct result of a sedentary lifestyle combined with poor diet. High-income nations also have a higher incidence of depression (Bromet et al. 2011). In contrast, low-income nations suffer significantly from malaria and tuberculosis.
How does health differ around the world? Some theorists differentiate among three types of countries: core nations, semi-peripheral nations, and peripheral nations. Core nations are those that we think of as highly developed or industrialized, semi-peripheral nations are those that are often called developing or newly industrialized, and peripheral nations are those that are relatively undeveloped. While the most pervasive issue in the U.S. healthcare system is affordable access to healthcare, other core countries have different issues, and semi-peripheral and peripheral nations are faced with a host of additional concerns. Reviewing the status of global health offers insight into the various ways that politics and wealth shape access to healthcare, and it shows which populations are most affected by health disparities.
Health in High-Income Nations
Obesity, which is on the rise in high-income nations, has been linked to many diseases, including cardiovascular problems, musculoskeletal problems, diabetes, and respiratory issues. According to the Organization for Economic Cooperation and Development (2011), obesity rates are rising in all countries, with the greatest gains being made in the highest-income countries. The United States has the highest obesity rate. Wallace Huffman and his fellow researchers (2006) contend that several factors are contributing to the rise in obesity in developed countries:
- Improvements in technology and reduced family size have led to a reduction of work to be done in household production.
- Unhealthy market goods, including processed foods, sweetened drinks, and sweet and salty snacks, are replacing home-produced goods.
- Leisure activities are growing more sedentary, for example, computer games, web surfing, and television viewing.
- More workers are shifting from active work (agriculture and manufacturing) to service industries.
- Increased access to passive transportation has led to more driving and less walking.
Obesity and weight issues have significant societal costs, including lower life expectancies and higher shared healthcare costs.
High-income countries also have higher rates of depression than less affluent nations. A recent study (Bromet et al. 2011) shows that the average lifetime prevalence of major depressive episodes in the ten highest-income countries in the study was 14.6 percent, this compared to 11.1 percent in the eight low- and middle-income countries. The researchers speculate that the higher rate of depression may be linked to the greater income inequality that exists in the highest-income nations.
Health in Low-Income Nations

In peripheral nations with low per-capita income, it is not the cost of healthcare that is the most pressing concern. Rather, low-income countries must manage such problems as infectious disease, high infant mortality rates, scarce medical personnel, and inadequate water and sewer systems. Such issues, which high-income countries rarely even think about, are central to the lives of most people in low-income nations. Due to such health concerns, low-income nations have higher rates of infant mortality and shorter average life spans.
One of the biggest contributors to medical issues in low-income countries is the lack of access to clean water and basic sanitation resources. According to a 2014 UNICEF report, almost half of the developing world’s population lacks improved sanitation facilities. The World Health Organization (WHO) tracks health-related data for 193 countries. In their 2011 World Health Statistics report, they document the following statistics:
- Globally, the rate of mortality for children under five was 60 per 1,000 live births. In low-income countries, however, that rate is almost double at 117 per 1,000 live births. In high-income countries, that rate is significantly lower than seven per 1,000 live births.
- The most frequent causes of death for children under five were pneumonia and diarrheal diseases, accounting for 18 percent and 15 percent, respectively. These deaths could be easily avoidable with cleaner water and more coverage of available medical care.
- The availability of doctors and nurses in low-income countries is one-tenth that of nations with a high income. Challenges in access to medical education and access to patients exacerbate this issue for would-be medical professionals in low-income countries (World Health Organization 2011).
13.3 Health in the United States
Learning Objectives
- Understand how social epidemiology can be applied to health in the United States
- Explain disparities in health based on gender, socioeconomic status, race, and ethnicity
- Give an overview of mental health and disability issues in the United States
- Explain the terms stigma and medicalization
Health in the United States is a complex and often contradictory issue. On the one hand, as one of the wealthiest nations, the United States fares well in health comparisons with the rest of the world. However, the United States also lags behind almost every industrialized country in terms of providing care to all its citizens. The following sections look at different aspects of health in the United States.
Health by Race and Ethnicity
When looking at the social epidemiology of the United States, it is hard to miss the disparities among races. The discrepancy between black and white Americans shows the gap clearly; in 2008, the average life expectancy for white males was approximately five years longer than for black males: 75.9 compared to 70.9. An even stronger disparity was found in 2007: in infant mortality, which is the number of deaths in a given time or place, the rate for blacks was nearly twice that of whites at 13.2 compared to 5.6 per 1,000 live births (U.S. Census Bureau 2011). According to a report from the Henry J. Kaiser Foundation (2007), African Americans also have a higher incidence of several other diseases and causes of mortality, from cancer to heart disease to diabetes. In a similar vein, it is important to note that ethnic minorities, including Mexican Americans and Native Americans, also have higher rates of these diseases and causes of mortality than whites.
Lisa Berkman (2009) notes that this gap started to narrow during the Civil Rights movement in the 1960s, but it began widening again in the early 1980s. What accounts for these perpetual disparities in health among different ethnic groups? Much of the answer lies in the level of healthcare that these groups receive. The National Healthcare Disparities Report (2010) shows that even after adjusting for insurance differences, racial and ethnic minority groups receive poorer quality of care and less access to care than dominant groups. The report identified these racial inequalities in care:
- Black Americans, American Indians, and Alaskan Natives received inferior care compared to White Americans for about 40 percent of measures.
- Asian ethnicities received inferior care for about 20 percent of measures.
- Among whites, Hispanic whites received 60 percent inferior care measures compared to non-Hispanic whites (Agency for Health Research and Quality 2010). When considering access to care, the figures were comparable.
Health by Socioeconomic Status
Discussions of health by race and ethnicity often overlap with discussions of health by socioeconomic status, since the two concepts are intertwined in the United States. As the Agency for Health Research and Quality (2010) notes, “racial and ethnic minorities are more likely than non-Hispanic whites to be poor or near-poor,” so much of the data pertaining to subordinate groups is also likely to be pertinent to low socioeconomic groups. Marilyn Winkleby and her research associates (1992) state that “one of the strongest and most consistent predictors of a person’s morbidity and mortality experience is that person’s socioeconomic status (SES). This finding persists across all diseases with few exceptions, continues throughout the entire lifespan, and extends across numerous risk factors for disease.” Morbidity is the incidence of disease.
It is important to remember that economics is only part of the SES picture; research suggests that education also plays an important role. Phelan and Link (2003) note that many behavior-influenced diseases like lung cancer (from smoking), coronary artery disease (from poor eating and exercise habits), and AIDS initially were widespread across SES groups. However, once information linking habits to disease was disseminated, these diseases decreased in high SES groups and increased in low SES groups. This illustrates the important role of education initiatives regarding a given disease, as well as possible inequalities in how those initiatives effectively reach different SES groups.
Health by Gender
Women are affected adversely both by unequal access to and institutionalized sexism in the healthcare industry. According to a recent report from the Kaiser Family Foundation, women experienced a decline in their ability to see needed specialists between 2001 and 2008. In 2008, one-quarter of females questioned the quality of their healthcare (Ranji and Salganico 2011). In this report, we also see the explanatory value of intersection theory. Feminist sociologist Patricia Hill Collins developed this theory, which suggests we cannot separate the effects of race, class, gender, sexual orientation, and other attributes. Further examination of the lack of confidence in the healthcare system by women, as identified in the Kaiser study, found, for example, women categorized as low income were more likely (32 percent compared to 23 percent) to express concerns about healthcare quality, illustrating the multiple layers of disadvantage caused by race and sex.
We can see an example of institutionalized sexism in the way that women are more likely than men to be diagnosed with certain kinds of mental disorders. Psychologist Dana Becker notes that 75 percent of all diagnoses of Borderline Personality Disorder (BPD) are for women according to the Diagnostic Statistical Manual of Mental Disorders. This diagnosis is characterized by instability of identity, mood, and behavior, and Becker argues that it has been used as a catch-all diagnosis for too many women. She further decries the pejorative connotation of the diagnosis, saying that it predisposes many people, both within and outside of the profession of psychotherapy, against women who have been so diagnosed (Becker).
Many critics also point to the medicalization of women’s issues as an example of institutionalized sexism. Medicalization refers to the process by which previously normal aspects of life are redefined as deviant and needing medical attention to remedy. Historically and contemporaneously, many aspects of women’s lives have been medicalized, including menstruation, pre-menstrual syndrome, pregnancy, childbirth, and menopause. The medicalization of pregnancy and childbirth has been particularly contentious in recent decades, with many women opting against the medical process and choosing more natural childbirth. Fox and Worts (1999) find that all women experience pain and anxiety during the birth process but that social support relieves both as effectively as medical support. In other words, medical interventions are no more effective than social ones at helping with the difficulties of pain and childbirth. Fox and Worts further found that women with supportive partners ended up with less medical intervention and fewer cases of postpartum depression. Of course, access to quality birth care outside the standard medical models may not be readily available to women of all social classes.
SOCIOLOGY IN THE REAL WORLD
Medicalization of Sleeplessness
How is your “sleep hygiene?” Sleep hygiene refers to the lifestyle and sleep habits that contribute to sleeplessness. Bad habits that can lead to sleeplessness include inconsistent bedtimes, lack of exercise, late-night employment, napping during the day, and sleep environments that include noise, lights, or screen time (National Institutes of Health 2011a).
According to the National Institute of Health, examining sleep hygiene is the first step in trying to solve a problem with sleeplessness.
For many people in the United States, however, making changes in sleep hygiene does not seem to be enough. According to a 2006 report from the Institute of Medicine, sleeplessness is an underrecognized public health problem affecting up to 70 million people. It is interesting to note that in the months (or years) after this report was released, advertising by the pharmaceutical companies behind Ambien, Lunesta, and Sepracor (three sleep aids) averaged $188 million weekly promoting these drugs (Gellene 2009).
According to a study in the American Journal of Public Health (2011), prescriptions for sleep medications increased dramatically from 1993 to 2007. While complaints of sleeplessness during doctor’s office visits more than doubled during this time, insomnia diagnoses increased more than sevenfold, from about 840,000 to 6.1 million. The authors of the study conclude that sleeplessness has been medicalized as insomnia, and that “insomnia may be a public health concern, but potential overtreatment with marginally effective, expensive medications with nontrivial side effects raises definite population health concerns” (Moloney, Konrad, and Zimmer 2011). Indeed, a study published in 2004 in the Archives of Internal Medicine shows that cognitive behavioral therapy, not medication, was the most effective sleep intervention (Jacobs, Pace-Schott, Stickgold, and Otto 2004).
A century ago, people who couldn’t sleep were told to count sheep. Now they pop a pill, and all those pills add up to a very lucrative market for the pharmaceutical industry. Is this industry behind the medicalization of sleeplessness, or is it just responding to a need?
Mental Health and Disability
The treatment received by those defined as mentally ill or disabled varies greatly from country to country. In the post-millennial United States, those of us who have never experienced such a disadvantage take for granted the rights our society guarantees for each citizen. We do not think about the relatively recent nature of the protections, unless, of course, we know someone constantly inconvenienced by the lack of accommodations or the misfortune of suddenly experiencing a temporary disability.
Mental Health
People with mental disorders (a condition that makes it more difficult to cope with everyday life) and people with mental illness (a severe, lasting mental disorder that requires long-term treatment) experience a wide range of effects.
According to the National Institute of Mental Health (NIMH), the most common mental disorders in the United States are anxiety disorders. Almost 18 percent of U.S. adults are likely to be affected in a single year, and 28 percent are likely to be affected over the course of a lifetime (National Institute of Mental Health 2005). It is important to distinguish between occasional feelings of anxiety and a true anxiety disorder. Anxiety is a normal reaction to stress that we all feel at some point, but anxiety disorders are feelings of worry and fearfulness that last for months at a time. Anxiety disorders include obsessive-compulsive disorder (OCD), panic disorders, posttraumatic stress disorder (PTSD), and both social and specific phobias.
The second most common mental disorders in the United States are mood disorders; roughly 10 percent of U.S. adults are likely to be affected yearly, while 21 percent are likely to be affected over the course of a lifetime (National Institute of Mental Health 2005). Major mood disorders are depression, bipolar disorder, and dysthymic disorder. Like anxiety, depression might seem like something that everyone experiences at some point, and it is true that most people feel sad or “blue” at times in their lives. A true depressive episode, however, is more than just feeling sad for a short period. It is a long-term, debilitating illness that usually needs treatment to cure. And bipolar disorder is characterized by dramatic shifts in energy and mood, often affecting the individual’s ability to carry out day-to-day tasks. Bipolar disorder used to be called manic depression because of the way people swing between manic and depressive episodes.
Depending on what definition is used, there is some overlap between mood disorders and personality disorders, which affect 9 percent of people in the United States yearly. The American Psychological Association publishes the Diagnostic and Statistical Manual on Mental Disorders (DSM), the DSM5-TR, which just came out in April 2022, defines a personality disorder as “an enduring pattern of inner experience and behavior that deviates markedly from the norms and expectations of the individual’s culture, is pervasive and inflexible, has an onset in adolescence or early adulthood, is stable over time, and leads to distress or impairment.” The personality disorders listed in the DSM5-TR are Paranoid personality disorder, Schizoid personality disorder, Schizotypal personality disorder, Antisocial personality disorder, Borderline personality disorder, Histrionic personality disorder, Narcissistic personality disorder, Avoidant personality disorder, Dependent personality disorder, Obsessive-compulsive personality disorder, Personality change due to another medical condition, and other specified personality disorder.

Another fairly commonly diagnosed mental disorder is Attention-Deficit/Hyperactivity Disorder (ADHD), which statistics suggest affects 9 percent of children and 8 percent of adults on a lifetime basis (National Institute of Mental Health 2005). ADHD is one of the most common childhood disorders, and it is marked by difficulty paying attention, difficulty controlling behavior, and hyperactivity. According to the American Psychological Association (APA), ADHD responds positively to stimulant drugs like Ritalin or Adderall, which helps people stay focused. However, there is some social debate over whether such drugs are being overprescribed (American Psychological Association). In fact, some critics question whether this disorder is really as widespread as it seems or if it is a case of overdiagnosis. According to the Centers for Disease Control and Prevention, only 5 percent of children have ADHD. However, approximately 11 percent of children ages four through seventeen have been diagnosed with ADHD as of 2011.
Autism Spectrum Disorders (ASD) have gained a lot of attention in recent years. The term ASD encompasses a group of developmental brain disorders that are characterized by “deficits in social interaction, verbal and nonverbal communication, and engagement in repetitive behaviors or interests” (National Institute of Mental Health). As with the personality disorders described above, the Diagnostic and Statistical Manual on Mental Disorders (DSM) 5th Edition-TR has these disorders listed under the Neurodevelopmental Disorders. Autism Spectrum Disorder, Attention-Deficit/Hyperactivity Disorder, Specific Learning Disorder, and Motor Disorders are now separate under the category of Neurodevelopmental Disorders.
The National Institute of Mental Health (NIMH) distinguishes between serious mental illness and other disorders. The key feature of serious mental illness is that it results in “serious functional impairment, which substantially interferes with or limits one or more major life activities” (National Institute of Mental Health). Thus, the characterization of “serious” refers to the effect of the illness (functional impairment), not the illness itself.
Disability

Disability refers to a reduction in one’s ability to perform everyday tasks. The World Health Organization makes a distinction between the various terms used to describe handicaps that are important to the sociological perspective. They use the term impairment to describe the physical limitations while reserving the term disability to refer to the social limitation.
Before the passage of the Americans with Disabilities Act (ADA) in 1990, people in the United States with disabilities were often excluded from opportunities and social institutions many of us take for granted. This occurred not only through employment and other kinds of discrimination but also through casual acceptance by most people in the United States of a world designed for the convenience of the able-bodied. Imagine being in a wheelchair and trying to use a sidewalk without the benefit of wheelchair-accessible curbs. Imagine a blind person trying to access information without the widespread availability of Braille. Imagine having limited motor control and being faced with a difficult-to-grasp round door handle. Issues like these are what the ADA tries to address. Ramps on sidewalks, Braille instructions, and more accessible door levers are all accommodations to help people with disabilities.
People with disabilities can be stigmatized by their illnesses. Stigmatization means their identity is spoiled; they are labeled as different, discriminated against, and sometimes even shunned. They are labeled (as an interactionist might point out) and ascribed a master status (as a functionalist might note), becoming “the blind girl” or “the boy in the wheelchair” instead of someone afforded a full identity by society. This can be especially true for people who are disabled due to mental illness or disorders.
As discussed in the section on mental health, many mental health disorders can be debilitating and can affect a person’s ability to cope with everyday life. This can affect social status, housing, and especially employment. According to the Bureau of Labor Statistics (2011), people with a disability had a higher rate of unemployment than people without a disability in 2010: 14.8 percent to 9.4 percent. This unemployment rate refers only to people actively looking for a job. In fact, eight out of ten people with a disability are considered “out of the labor force;” that is, they do not have jobs and are not looking for them. The combination of this population and the high unemployment rate leads to an employment-population ratio of 18.6 percent among those with disabilities. The employment-population ratio for people without disabilities was much higher, at 63.5 percent (U.S. Bureau of Labor Statistics 2011).
SOCIOLOGY IN THE REAL WORLD
Obesity: The Last Acceptable Prejudice

What is your reaction to the picture above? Compassion? Fear? Disgust? Many people will look at this picture and make negative assumptions about the man based on his weight. According to a study from the Yale Rudd Center for Food Policy and Obesity, large people are the object of “widespread negative stereotypes that overweight and obese persons are lazy, unmotivated, lacking in self-discipline, less competent, noncompliant, and sloppy” (Puhl and Heuer 2009).
Historically, both in the United States and elsewhere, it was considered acceptable to discriminate against people based on prejudiced opinions. Even after slavery was abolished in 1865, the next 100 years of U.S. history saw institutionalized racism and prejudice against black people. In an example of stereotype interchangeability, the same insults that are flung today at the overweight and obese population (lazy, for instance) have been flung at various racial and ethnic groups in earlier history. Of course, no one gives voice to these kinds of views in public now, except when talking about obese people.
Why is it considered acceptable to feel prejudice toward—even to hate—obese people? Puhl and Heuer suggest that these feelings stem from the perception that obesity is preventable through self-control, a better diet, and more exercise. Highlighting this contention is the fact that studies have shown that people’s perceptions of obesity are more positive when they think the obesity was caused by non-controllable factors like biology (a thyroid condition, for instance) or genetics.
Even with some understanding of non-controllable factors that might affect obesity, obese people are still subject to stigmatization. Puhl and Heuer’s study is one of many that document discrimination at work, in the media, and even in the medical profession. Obese people are less likely to get into college than thinner people, and they are less likely to succeed at work.
Stigmatization of obese people comes in many forms, from the seemingly benign to the potentially illegal. In movies and television shows, overweight people are often portrayed negatively or as stock characters who are the butt of jokes. One study of children’s movies found that “obesity was equated with negative traits (evil, unattractive, unfriendly, cruel) in 64 percent of the most popular children’s videos. In 72 percent of the videos, characters with thin bodies had desirable traits, such as kindness or happiness” (Hines and Thompson 2007). In movies and television for adults, the negative portrayal is often meant to be funny. “Fat suits”—inflatable suits that make people look obese—are commonly used in a way that perpetuates negative stereotypes. Think about the way you have seen obese people portrayed in movies and on television; now think of any other subordinate group being openly denigrated in such a way. It is difficult to find a parallel example.
13.4 Comparative Health and Medicine
Learning Objectives
- Explain the different types of health care available in the United States
- Compare the health care system of the United States with that of other countries
There are broad, structural differences among the healthcare systems of different countries. In core nations, those differences might arise in the administration of healthcare, while the care itself is similar. In peripheral and semi-peripheral countries, a lack of basic healthcare administration can be the defining feature of the system. Most countries rely on some combination of modern and traditional medicine. In core countries with large investments in technology, research, and equipment, the focus is usually on modern medicine, with traditional (also called alternative or complementary) medicine playing a secondary role. In the United States, for instance, the American Medical Association (AMA) resolved to support the incorporation of complementary and alternative medicine in medical education. In developing countries, even quickly modernizing ones like China, traditional medicine (often understood as “complementary” by the Western world) may still play a larger role.
U.S. Healthcare
U.S. healthcare coverage can broadly be divided into two main categories: public healthcare (government-funded) and private healthcare (privately funded).
The two main publicly funded healthcare programs are Medicare, which provides health services to people over sixty-five years old as well as people who meet other standards for disability, and Medicaid, which provides services to people with very low incomes who meet other eligibility requirements. Other government-funded programs include service agencies focused on Native Americans (the Indian Health Service), Veterans (the Veterans Health Administration), and children (the Children’s Health Insurance Program). A controversial issue in 2011 was a proposed constitutional amendment requiring a balanced federal budget, which would almost certainly require billions of dollars in cuts to these programs. As discussed below, the United States already has a significant problem with a lack of healthcare coverage for many individuals; if these budget cuts pass, the already heavily burdened programs are sure to suffer, and so are the people they serve (Kogan 2011).
The U.S. Census (2011) divides private insurance into employment-based insurance and direct-purchase insurance. Employment-based insurance is health plan coverage that is provided in whole or in part by an employer or union; it can cover just the employee or the employee and his or her family. Direct purchase insurance is coverage that an individual buys directly from a private company.
With all these insurance options, insurance coverage must be almost universal, right? Unfortunately, the U.S. Census Current Population Survey of 2013 shows that 18 percent of people in the United States have no health insurance at all. Equally alarming, a study by the Commonwealth Fund shows that in 2010, 81 million adults were either uninsured or underinsured—that is, people who pay at least 10 percent of their income on healthcare costs not covered by insurance or, for low-income adults, those whose medical expenses or deductibles are at least 5 percent of their income (Schoen, Doty, Robertson, and Collins 2011). The Commonwealth study further reports that while underinsurance has historically been an issue that low-income families faced, today it is affecting middle-income families more and more.
Why are so many people uninsured or underinsured? Skyrocketing healthcare costs are part of the issue. Many people cannot afford private health insurance, but their income level is not low enough to meet eligibility standards for government-supported insurance. Further, even for those who are eligible for Medicaid, the program is less than perfect. Many physicians refuse to accept Medicaid patients, citing low payments and extensive paperwork (Washington University Center for Health Policy, n.d.).
Healthcare in the United States is a complex issue, and it will only get more so with the continued enactment of the Patient Protection and Affordable Care Act (PPACA) of 2010. This act, sometimes called “Obamacare” for its most noted advocate, President Barack Obama, represents large-scale federal reform of the United States healthcare system. The PPACA aims to address some of the biggest flaws of the current healthcare system. It expands eligibility to programs like Medicaid and CHIP, helps guarantee insurance coverage for people with pre-existing conditions, and establishes regulations to make sure that the premium funds collected by insurers and care providers go directly to medical care. It also includes an individual mandate, which requires everyone to have insurance coverage by 2014 or pay a penalty. A series of provisions, including significant subsidies, are intended to address the discrepancies in income that are currently contributing to high rates of uninsurance and underinsurance. In 2012 the U.S. Supreme Court upheld the constitutionality of the PPACA’s individual mandate. According to Blumenthal (2014), 20 million people in the United States have gained health insurance under PPACA. This lowers the number of uninsured people to 13 percent.

The PPACA remains contentious. The Supreme Court ruled in the case of National Federation of Independent Businesses v. Sebelius in 2012, that states cannot be forced to participate in the PPACA’s Medicaid expansion. This ruling has opened the door to challenges to the PPACA in Congress and the Federal courts, some state governments, conservative groups, and independent businesses. A concern to public health officials is fear among some parents that certain vaccines such as the measles, mumps, and rubella (MMR) vaccine are linked to a higher risk of autism. According to Uchiyama et al (2007), there is no link between MMR and autism. However, fear of this perceived link pushes some parents to refuse the MMR vaccine for their children.
An additional issue in U.S. healthcare has been the push to legalize marijuana in some states. As of this writing, twenty-three states and the District of Columbia allow the use of medical cannabis (Borgelt 2013). Marijuana reform appears to partly be the repackaging of marijuana from a drug to a “medicine.” Medical evidence has demonstrated positive responses in the treatment of a variety of illnesses, from some cancers to glaucoma and epilepsy. Concerns regarding the cost and long-term effects of the PPACA continue to be discussed at various societal levels.
Healthcare Elsewhere
Clearly, healthcare in the United States has some areas for improvement. But how does it compare to healthcare in other countries? Many people in the United States are fond of saying that this country has the best healthcare in the world, and while it is true that the United States has a higher quality of care available than many peripheral or semi-peripheral nations, it is not necessarily the “best in the world.” In a report on how U.S. healthcare compares to that of other countries, researchers found that the United States does “relatively well in some areas—such as cancer care—and less well in others—such as mortality from conditions amenable to prevention and treatment” (Docteur and Berenson 2009).
One critique of the Patient Protection and Affordable Care Act is that it will create a system of socialized medicine, a term that for many people in the United States has negative connotations lingering from the Cold War era and earlier. Under a socialized medicine system, the government owns and runs the system. It employs the doctors, nurses, and other staff, and it owns and runs the hospitals (Klein 2009). The best example of socialized medicine is in Great Britain, where the National Health System (NHS) gives free healthcare to all its residents. And despite some U.S. citizens’ knee-jerk reaction to any healthcare changes that hint at socialism, the United States has one socialized system with the Veterans Health Administration.
It is important to distinguish between socialized medicine, in which the government owns the healthcare system, and universal healthcare, which is simply a system that guarantees healthcare coverage for everyone. Germany, Singapore, and Canada all have universal healthcare. People often look to Canada’s universal healthcare system, Medicare, as a model for the system. In Canada, healthcare is publicly funded and is administered by the separate provincial and territorial governments. However, the care itself comes from private providers. This is the main difference between universal healthcare and socialized medicine. The Canada Health Act of 1970 required that all health insurance plans must be “available to all eligible Canadian residents, comprehensive in coverage, accessible, portable among provinces, and publicly administered” (International Health Systems Canada 2010).
Heated discussions about the socialization of medicine and managed-care options seem frivolous when compared with the issues of healthcare systems in developing or underdeveloped countries. In many countries, per capita income is so low, and governments are so fractured, that healthcare as we know it is virtually non-existent. Care that people in developed countries take for granted—like hospitals, healthcare workers, immunizations, antibiotics, and other medications, and even sanitary water for drinking and washing—is unavailable to much of the population. Organizations like Doctors Without Borders, UNICEF, and the World Health Organization have played an important role in helping these countries get their most basic health needs met.
WHO, which is the health arm of the United Nations, set eight Millennium Development Goals (MDGs) in 2000 with the aim of reaching these goals by 2015. Some of the goals deal more broadly with the socioeconomic factors that influence health, but MDGs 4, 5, and 6 all relate specifically to large-scale health concerns, the likes of which most people in the United States will never contemplate. MDG 4 plans to reduce child mortality, MDG 5 aims to improve maternal health, and MDG 6 strives to combat HIV/AIDS, malaria, and other diseases. The goals may not seem particularly dramatic, but the numbers behind them show how serious they are.
For MDG 4, the WHO reports that 2009 infant mortality rates in “children under 5 years old in the WHO African Region (127 per 1000 live births) and in low-income countries (117 per 1000 live births) [had dropped], but they were still higher than the 1990 global level of 89 per 1000 live births” (World Health Organization 2011). The fact that these deaths could have been avoided through appropriate medicine and clean drinking water shows the importance of healthcare.
Much progress has been made on MDG 5, with maternal deaths decreasing by 34 percent. However, almost all maternal deaths occurred in developing countries, with the African region still experiencing high numbers (World Health Organization 2011).
On MDG 6, the WHO is seeing some decreases in per capita incidence rates of malaria, tuberculosis, HIV/AIDS, and other diseases. However, the decreases are often offset by population increases (World Health Organization 2011). Again, the lowest-income countries, especially in the African region, experience the worst problems with disease. An important component of disease prevention and control is epidemiology, or the study of the incidence, distribution, and possible control of diseases. Fear of Ebola contamination, primarily in Western Africa but also to a smaller degree in the United States, became national news in the summer and fall of 2014.
13.5 Theoretical Perspectives on Health and Medicine
Learning Objectives
- Apply functionalist, conflict theorist, and interactionist perspectives to health issues
Each of the three major theoretical perspectives approaches the topics of health, illness, and medicine differently. You may prefer just one of the theories that follow, or you may find that combining theories and perspectives provides a fuller picture of how we experience health and wellness.
Functionalism
According to the functionalist perspective, health is vital to the stability of society, and therefore sickness is a sanctioned form of deviance. Talcott Parsons (1951) was the first to discuss this in terms of the sick role: patterns of expectations that define appropriate behavior for the sick and for those who take care of them.
According to Parsons, the sick person has a specific role with both rights and responsibilities. To start with, she has not chosen to be sick and should not be treated as responsible for her condition. The sick person also has the right to be exempt from normal social roles; she is not required to fulfill the obligations of a well person and can avoid her normal responsibilities without censure. However, this exemption is temporary and relative to the severity of the illness. The exemption also requires legitimation by a physician; that is, a physician must certify that the illness is genuine.
The responsibility of the sick person is twofold: to try to get well and to seek technically competent help from a physician. If the sick person stays ill longer than is appropriate (malingers), she may be stigmatized.
Parsons argues that since the sick are unable to fulfill their normal societal roles, their sickness weakens society. Therefore, it is sometimes necessary for various forms of social control to bring the behavior of a sick person back in line with normal expectations. In this model of health, doctors serve as gatekeepers, deciding who is healthy and who is sick—a relationship in which the doctor has all the power. But is it appropriate to allow doctors so much power over deciding who is sick? And what about people who are sick but are unwilling to leave their positions for any number of reasons (personal/social obligations, financial need, or lack of insurance, for instance)?
Conflict Perspective
Theorists using the conflict perspective suggest that issues with the healthcare system, as with most other social problems, are rooted in capitalist society. According to conflict theorists, capitalism and the pursuit of profit lead to the commodification of health: the changing of something not generally thought of as a commodity into something that can be bought and sold in a marketplace. In this view, people with money and power—the dominant group—are the ones who make decisions about how the healthcare system will be run. They, therefore, ensure that they will have healthcare coverage, while simultaneously ensuring that subordinate groups stay subordinate through lack of access. This creates significant healthcare—and health—disparities between the dominant and subordinate groups.
Alongside the health disparities created by class inequalities, there are a number of health disparities created by racism, sexism, ageism, and heterosexism. When health is a commodity, the poor are more likely to experience illness caused by poor diet, to live and work in unhealthy environments, and are less likely to challenge the system. In the United States, a disproportionate number of racial minorities also have less economic power, so they bear a great deal of the burden of poor health. It is not only the poor who suffer from the conflict between dominant and subordinate groups. For many years now, homosexual couples have been denied spousal benefits, either in the form of health insurance or in terms of medical responsibility. Further adding to the issue, doctors hold a disproportionate amount of power in the doctor/patient relationship, which provides them with extensive social and economic benefits.
While conflict theorists are accurate in pointing out certain inequalities in the healthcare system, they do not give enough credit to medical advances that would not have been made without an economic structure to support and reward researchers: a structure dependent on profitability. Additionally, in their criticism of the power differential between doctor and patient, they are perhaps dismissive of the hard-won medical expertise possessed by doctors and not patients, which renders a truly egalitarian relationship more elusive.
Symbolic Interactionism
According to theorists working in this perspective, health and illness are both socially constructed. As we discussed in the beginning of the chapter, interactionists focus on the specific meanings and causes people attribute to illness. The term medicalization of deviance refers to the process that changes “bad” behavior into “sick” behavior. A related process is demedicalization, in which “sick” behavior is normalized again. Medicalization and demedicalization affect who responds to the patient, how people respond to the patient, and how people view the personal responsibility of the patient (Conrad and Schneider 1992).
An example of medicalization is illustrated by the history of how our society views alcohol and alcoholism. During the nineteenth century, people who drank too much were considered bad, lazy people. They were called drunks, and it was not uncommon for them to be arrested or run out of a town. Drunks were not treated in a sympathetic way because, at that time, it was thought that it was their own fault that they could not stop drinking. During the latter half of the twentieth century, however, people who drank too much were increasingly defined as alcoholics: people with a disease or a genetic predisposition to addiction who were not responsible for their drinking. With alcoholism defined as a disease and not a personal choice, alcoholics came to be viewed with more compassion and understanding. Thus, “badness” was transformed into “sickness.”
There are numerous examples of demedicalization in history as well. During the Civil War era, slaves who frequently ran away from their owners were diagnosed with a mental disorder called drapetomania. This has since been reinterpreted as a completely appropriate response to being enslaved. A more recent example is homosexuality, which was labeled a mental disorder or a sexual orientation disturbance by the American Psychological Association until 1973.
While interactionism does acknowledge the subjective nature of diagnosis, it is important to remember who most benefits when a behavior becomes defined as illness. Pharmaceutical companies make billions treating illnesses such as fatigue, insomnia, and hyperactivity that may not actually be illnesses in need of treatment but opportunities for companies to make more money.
Key Terms
- anxiety disorders
- feelings of worry and fearfulness that last for months at a time
- commodification
- the changing of something not generally thought of as a commodity into something that can be bought and sold in a marketplace
- contested illnesses
- illnesses that are questioned or considered questionable by some medical professionals
- demedicalization
- the social process that normalizes “sick” behavior
- disability
- a reduction in one’s ability to perform everyday tasks; the World Health Organization notes that this is a social limitation
- epidemiology
- the study of the incidence, distribution, and possible control of diseases
- impairment
- the physical limitations a less-able person faces
- individual mandate
- a government rule that requires everyone to have insurance coverage or they will have to pay a penalty
- legitimation
- the act of a physician certifying that an illness is genuine
- medical sociology
- the systematic study of how humans manage issues of health and illness, disease and disorders, and healthcare for both the sick and the healthy
- medicalization
- the process by which aspects of life that were considered bad or deviant are redefined as sickness and needing medical attention to remedy
- medicalization of deviance
- the process that changes “bad” behavior into “sick” behavior
- mood disorders
- long-term, debilitating illnesses like depression and bipolar disorder
- morbidity
- the incidence of disease
- mortality
- the number of deaths in a given time or place
- personality disorders
- disorders that cause people to behave in ways that are seen as abnormal to society but seem normal to them
- private healthcare
- health insurance that a person buys from a private company; private healthcare can either be employer-sponsored or direct-purchase
- public healthcare
- health insurance that is funded or provided by the government
- sick role
- the pattern of expectations that define appropriate behavior for the sick and for those who take care of them
- social epidemiology
- the study of the causes and distribution of diseases
- socialized medicine
- when the government owns and runs the entire healthcare system
- stereotype interchangeability
- stereotypes that don’t change and that get recycled for application to a new subordinate group
- stigmatization
- the act of spoiling someone’s identity; they are labeled as different, discriminated against, and sometimes even shunned due to an illness or disability
- stigmatization of illness
- illnesses that are discriminated against and whose sufferers are looked down upon or even shunned by society
- underinsured
- people who spend at least 10 percent of their income on healthcare costs that are not covered by insurance
- universal healthcare
- a system that guarantees healthcare coverage for everyone
Section Summary
13.1 The Social Construction of Health
Medical sociology is the systematic study of how humans manage issues of health and illness, disease and disorders, and healthcare for both the sick and the healthy. The social construction of health explains how society shapes and is shaped by medical ideas.
13.2 Global Health
Social epidemiology is the study of the causes and distribution of diseases. From a global perspective, the health issues of high-income nations tend toward diseases like cancer as well as those that are linked to obesity, like heart disease, diabetes, and musculoskeletal disorders. Low-income nations are more likely to contend with infectious diseases, high infant mortality rates, scarce medical personnel, and inadequate water and sanitation systems.
13.3 Health in the United States
Although people in the United States are generally in good health compared to less developed countries, the United States is still facing challenging issues such as the prevalence of obesity and diabetes. Moreover, people in the United States of historically disadvantaged racial groups, ethnicities, socioeconomic statuses, and genders experience lower levels of healthcare. Mental health and disability are health issues that are significantly impacted by social norms.
13.4 Comparative Health and Medicine
There are broad, structural differences among the healthcare systems of different countries. In core nations, those differences include publicly funded healthcare, privately funded healthcare, and combinations of both. In peripheral and semi-peripheral countries, a lack of basic healthcare administration can be the defining feature of the system.
13.5 Theoretical Perspectives on Health and Medicine
While the functionalist perspective looks at how health and illness fit into a fully functioning society, the conflict perspective is concerned with how health and illness fit into the oppositional forces in society. The interactionist perspective is concerned with how social interactions construct ideas of health and illness.
Section Quiz
13.1 The Social Construction of Health
1. Who determines which illnesses are stigmatized?
- Therapists
- The patients themselves
- Society
- All of the above
2. Chronic fatigue syndrome is an example of _______________.
- a stigmatized disease
- a contested illness
- a disability
- demedicalization
3. The Rating of Perceived Exertion (RPE) is an example of ________________
- the social construction of health
- medicalization
- disability accommodations
- a contested illness
13.2 Global Health
- The study of why some diseases are stigmatized and others are not
- The study of why diseases spread
- The study of the mental health of a society
- The study of the causes and distribution of diseases
5. Core nations are also known as __________________
- high-income nations
- newly industrialized nations
- low-income nations
- developing nations
6. Many deaths in high-income nations are linked to __________________
- lung cancer
- obesity
- mental illness
- lack of clean water
7. According to the World Health Organization, what was the most frequent cause of death for children under five in low-income countries?
- Starvation
- Thirst
- Pneumonia and diarrheal diseases
- All of the above
13.3 Health in the United States
- The life expectancy of black males in the United States is approximately five years shorter than for white males.
- The infant mortality rate for blacks in the United States is almost double than it is for white.
- Blacks have lower cancer rates than whites.
- Hispanics have worse access to care than non-Hispanic whites.
9. The process by which aspects of life that were considered bad or deviant are redefined as sickness and needing medical attention to remedy is called:
- deviance
- medicalization
- demedicalization
- intersection theory
10. What are the most commonly diagnosed mental disorders in the United States?
- ADHD
- Mood disorders
- Autism spectrum disorders
- Anxiety disorders
11. Sidewalk ramps and Braille signs are examples of _______________.
- disabilities
- accommodations required by the Americans with Disabilities Act
- forms of accessibility for people with disabilities
- both b and c
12. The high unemployment rate among the disabled may be a result of ____________.
- medicalization
- obesity
- stigmatization
- all of the above
13.4 Comparative Health and Medicine
- Medicaid
- Medicare
- Veterans Health Administration
- All of the above
14. Which program is an example of socialized medicine?
- Canada’s system
- The United States’ Veterans Health Administration
- The United States’ new system under the Patient Protection and Affordable Care Act
- Medicaid
15. What does the individual mandate provision of the 2010 U.S. healthcare reform do?
- Requires everyone to buy insurance from the government
- Requires everyone to sign up for Medicaid
- Requires everyone to have insurance or pay a penalty
- None of the above
16. Great Britain’s healthcare system is an example of ______________
- socialized medicine
- private healthcare
- single-payer private healthcare
- universal private healthcare
17. What group created the Millennium Development Goals?
- UNICEF
- The Kaiser Family Foundation
- Doctors Without Borders
- The World Health Organization
13.5 Theoretical Perspectives on Health and Medicine
18. Which of the following is not part of the rights and responsibilities of a sick person under the functionalist perspective?
- The sick person is not responsible for his condition.
- The sick person must try to get better.
- The sick person can take as long as she wants to get better.
- The sick person is exempt from the normal duties of society.
19. The class, race, and gender inequalities in our healthcare system support the _____________ perspective.
- conflict
- interactionist
- functionalist
- all of the above
20. The removal of homosexuality from the DSM is an example of ____________.
- medicalization
- deviance
- interactionist theory
- demedicalization
Short Answer
13.1 The Social Construction of Health
1. Pick a common illness and describe which parts of it are medically constructed, and which parts are socially constructed.
2. What diseases are the most stigmatized? Which are the least? Is this different in different cultures or social classes?
13.2 Global Health
13.3 Health in the United States
13.4 Comparative Health and Medicine
13.5 Theoretical Perspectives on Health and Medicine
10. What examples of medicalization and demedicalization can you think of?
Further Research
13.1 The Social Construction of Health
Spend some time on the two websites below. How do they present differing views of the vaccination controversy? Freedom of Choice Is Not Free: Vaccination News: http://openstax.org/l/vaccination_news; and Shot by Shot: Stories of Vaccine-Preventable Illnesses: http://openstax.org/l/shot_by_shot
13.2 Global Health
Study this map on global life expectancies: http://openstax.org/l/global_life_expectancies. What trends do you notice?
13.3 Health in the United States
Is ADHD a valid diagnosis and disease? Some think it is not. This article discusses the history of the issue: http://openstax.org/l/ADHD_controversy
13.4 Comparative Health and Medicine
Project Mosquito Net says that mosquito nets sprayed with insecticide can reduce childhood malaria deaths by half. Read more at http://openstax.org/l/project_mosquito_net
13.5 Theoretical Perspectives on Health and Medicine
Should alcoholism and other addictions be medicalized? Read and watch a dissenting view: http://openstax.org/l/addiction_medicalization
References
Introduction to Health and Medicine
ABC News Health News. “Ebola in America, Timeline of a Deadly Virus.” Retrieved Oct. 23rd, 2014 (http://abcnews.go.com/Health/ebola-america-timeline/story?id=26159719).
Centers for Disease Control. 2011b. “Pertussis.” The Centers for Disease Control and Prevention. Retrieved December 15, 2011 (http://www.cdc.gov/pertussis/outbreaks.html).
Centers for Disease Control. 2022. “Covid 19 Museum Timeline” Retrieved May 14, 2022. https://www.cdc.gov/museum/timeline/covid19.html/
Conrad, Peter, and Kristin Barker. 2010. “The Social Construction of Illness: Key Insights and Policy Implications.” Journal of Health and Social Behavior 51:67–79.
COVID-19. 2022. WHO Coronavirus (COVID-19) Dashboard – Retrieved May 14, 2022 https://www.covid19.who.int
CNN. 2011. “Retracted Autism Study an ‘Elaborate Fraud,’ British Journal Finds.” CNN, January 5. Retrieved December 16, 2011 (http://www.cnn.com/2011/HEALTH/01/05/autism.vaccines/index.html).
Devlin, Kate. 2008. “Measles worry MMR as vaccination rates stall.” The Telegraph, September 24. Retrieved January 19, 2012 (http://www.telegraph.co.uk/news/uknews/3074023/Measles-worries-as-MMR-vaccination-rates-stall.html).
Sugerman, David E., Albert E. Barskey, Maryann G. Delea, Ismael R. Ortega-Sanchez, Daoling Bi, Kimberly J. Ralston, Paul A. Rota, Karen Waters-Montijo, and Charles W. LeBaron. 2010. “Measles Outbreak in a Highly Vaccinated Population, San Diego, 2008: Role of the Intentionally Undervaccinated.” Pediatrics 125(4):747–755. Retrieved December 16, 2011 (http://www.pediatricsdigest.mobi/content/125/4/747.full).
World Health Organization. 2014. “Global Alert and Response.” Retrieved Oct. 23rd 2014 (http://www.who.int/csr/disease/ebola/en/).
Zacharyczuk, Colleen. 2011. “Myriad causes contributed to California pertussis outbreak.” Thorofar, NJ: Pediatric Supersite. Retrieved December 16, 2011 (http://www.pediatricsupersite.com/view.aspx?rid=90516).
13.1 The Social Construction of Health
Begos, Kevin. 2011. “Pinkwashing For Breast Cancer Awareness Questioned.” Retrieved December 16, 2011 (http://www.huffingtonpost.com/2011/10/11/breast-cancer-pink-pinkwashing_n_1005906.html).
Centers for Disease Control. 2011a. “Perceived Exertion (Borg Rating of Perceived Exertion Scale).” Centers for Disease Control and Prevention. Retrieved December 12, 2011 (http://www.cdc.gov/physicalactivity/everyone/measuring/exertion.html).
Conrad, Peter, and Kristin Barker. 2010. “The Social Construction of Illness: Key Insights and Policy Implications.” Journal of Health and Social Behavior 51:67–79.
Goffman, Erving. 1963. Stigma: Notes on the Management of Spoiled Identity. London: Penguin.
Hutchison, Courtney. 2010. “Fried Chicken for the Cure?” ABC News Medical Unit. Retrieved December 16, 2011 (http://abcnews.go.com/Health/Wellness/kfc-fights-breast-cancer-fried-chicken/story?id=10458830#.Tutz63ryT4s).
Sartorius, Norman. 2007. “Stigmatized Illness and Health Care.” The Croatian Medical Journal 48(3):396–397. Retrieved December 12, 2011 (http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2080544/).
Think Before You Pink. 2012. “Before You Buy Pink.” Retrieved December 16, 2011 (http://thinkbeforeyoupink.org/?page_id=13).
“Vaccines and Immunizations.” 2011. The Centers for Disease Control and Prevention. Retrieved December 16, 2011 (http://www.cdc.gov/vaccines/default.htm).
World Health Organization. n.d. “Definition of Health.” Retrieved December 12, 2011 (http://www.who.int/about/definition/en/print.html).
World Health Organization: “Health Promotion Glossary Update.” Retrieved December 12, 2011 (http://www.who.int/healthpromotion/about/HPR%20Glossary_New%20Terms.pdf).
13.2 Global Health
Bromet et al. 2011. “Cross-National Epidemiology of DSM-IV Major Depressive Episode.” BMC Medicine 9:90. Retrieved December 12, 2011 (http://www.biomedcentral.com/1741-7015/9/90).
Huffman, Wallace E., Sonya Kostova Huffman, AbebayehuTegene, and KyrreRickertsen. 2006. “The Economics of Obesity-Related Mortality among High Income Countries” International Association of Agricultural Economists. Retrieved December 12, 2011 (http://purl.umn.edu/25567).
Organization for Economic Cooperation and Development. 2011. Health at a Glance 2011: OECD Indicators. OECD Publishing. Retrieved December 12, 2011 (http://dx.doi.org/10.1787/health_glance-2011-en).
UNICEF. 2011. “Water, Sanitation and Hygiene.” Retrieved December 12, 2011 (http://www.unicef.org/wash).
World Health Organization. 2011. “World Health Statistics 2011.” Retrieved December 12, 2011 (http://www.who.int/gho/publications/world_health_statistics/EN_WHS2011_Part1.pdf).
13.3 Health in the United States
Agency for Health Research and Quality. 2010. “Disparities in Healthcare Quality Among Racial and Ethnic Minority Groups.” Agency for Health Research and Quality. Retrieved December 13, 2011 (http://www.ahrq.gov/qual/nhqrdr10/nhqrdrminority10.htm).
American Psychiatric Association. 2022. DSM-5TR “Personality Disorder” pg. 733.
American Psychiatric Association. 2022. DSM-5TR “Neurodevelopmental Disorders” Autism Spectrum Disorder p. 56.
American Psychiatric Association. 2022. DSM-5TR “Neurodevelopment Disorders: Attention-Deficit/Hyperactivity Disorder” p.68.
American Psychological Association. 2011a. “A 09 Autism Spectrum Disorder.” American Psychiatric Association DSM-5 Development. Retrieved December 14, 2011.
American Psychological Association. 2011b. “Personality Traits.” American Psychiatric Association DSM-5 Development. Retrieved December 14, 2011.
American Psychological Association. n.d. “Understanding the Ritalin Debate.” American Psychological Association. Retrieved December 14, 2011 (http://www.apa.org/topics/adhd/ritalin-debate.aspx).
Becker, Dana. n.d. “Borderline Personality Disorder: The Disparagement of Women through Diagnosis.” Retrieved December 13, 2011 (http://www.awpsych.org/index.php?option=com_content&view=article&id=109&catid=74&Itemid=126).
Berkman, Lisa F. 2009. “Social Epidemiology: Social Determinants of Health in the United States: Are We Losing Ground?” Annual Review of Public Health 30:27–40.
Blumenthal, David, and Sarah R. Collins. 2014 “Health Care Coverage under the Affordable Care Act—a Progress Report.” New England Journal of Medicine 371 (3): 275–81. Retrieved December 16, 2014 (https://owl.english.purdue.edu/owl/resource/717/04/).
Fox, B., and D. Worts. 1999. “Revisiting the Critique of Medicalized Childbirth: A Contribution to the Sociology of Birth.” Gender and Society 13(3):326–346.
Gellene, Denise. 2009. “Sleeping Pill Use Grows as Economy Keeps People up at Night.” Retrieved December 16, 2011 (http://articles.latimes.com/2009/mar/30/health/he-sleep30).
Hines, Susan M., and Kevin J. Thompson. 2007. “Fat Stigmatization in Television Shows and Movies: A Content Analysis.” Obesity 15:712–718. Retrieved December 15, 2011 (http://onlinelibrary.wiley.com/doi/10.1038/oby.2007.635/full).
Institute of Medicine. 2006. Sleep Disorders and Sleep Deprivation: An Unmet Public Health Problem. Washington DC: National Academies Press.
Jacobs, Gregg D., Edward F. Pace-Schott, Robert Stickgold, and Michael W. Otto. 2004. “Cognitive Behavior Therapy and Pharmacotherapy for Insomnia: A Randomized Controlled Trial and Direct Comparison.” Archives of Internal Medicine 164(17):1888–1896. Retrieved December 16, 2011 (http://archinte.jamanetwork.com/article.aspx?articleid=217394).
James, Cara et al. 2007. “Key Facts: Race, Ethnicity & Medical Care.” The Henry J. Kaiser Family Foundation. Retrieved December 13, 2011 (http://www.kff.org/minorityhealth/upload/6069-02.pdf).
Moloney, Mairead Eastin, Thomas R. Konrad, and Catherine R. Zimmer. 2011. “The Medicalization of Sleeplessness: A Public Health Concern.” American Journal of Public Health101:1429–1433.
National Institute of Mental Health. 2005. “National Institute of Mental Health Statistics.” Retrieved December 14, 2011 (http://www.nimh.nih.gov/statistics/index.shtml).
National Institutes of Health. 2011a. “Insomnia.” The National Institute of Health. Retrieved December 16, 2011 (http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001808/).
National Institutes of Health. 2011b. “What is Autism Spectrum Disorder (ASD)?” National Institute of Mental Health. Retrieved December 14, 2011 (http://www.nimh.nih.gov/health/publications/a-parents-guide-to-autism-spectrum-disorder/what-is-autism-spectrum-disorder-asd.shtml).
Phelan, Jo C., and Bruce G. Link. 2001. “Conceptualizing Stigma” Annual Review of Sociology 27:363–85. Retrieved December 13, 2011 (http://www.heart-intl.net/HEART/Legal/Comp/ConceptualizingStigma.pdf).
Phelan, Jo C., and Bruce G. Link. 2003. “When Income Affects Outcome: Socioeconomic Status and Health.” Research in Profile:6. Retrieved December 13, 2011 (http://www.investigatorawards.org/downloads/research_in_profiles_iss06_feb2003.pdf).
Puhl, Rebecca M., and Chelsea A. Heuer. 2009. “The Stigma of Obesity: A Review and Update.” Nature Publishing Group. Retrieved December 15, 2011 (http://www.yaleruddcenter.org/resources/upload/docs/what/bias/WeightBiasStudy.pdf).
Ranji, Usha, and Alina Salganico. 2011. “Women’s Health Care Chartbook: Key Findings from the Kaiser Women’s Health Survey.” The Henry J. Kaiser Family Foundation. Retrieved December 13, 2011 (http://www.kff.org/womenshealth/upload/8164.pdf).
Scheff, Thomas. 1963. Being Mentally Ill: A Sociological Theory. Chicago, IL: Aldine.
Szasz, Thomas. 1961. The Myth of Mental Illness: Foundations of a Theory of Personal Conduct. New York, NY: Harper Collins.
U.S. Census Bureau. 2011. “Statistical Abstract of the United States: 2012.” 131st ed. Washington, DC. Retrieved December 13, 2011 (http://www.census.gov/compendia/statab).
U.S. Bureau of Labor Statistics. 2011. “Persons with a Disability: Labor Force Characteristics News Release.” Bureau of Labor Statistics. Retrieved December 14, 2011 (http://www.bls.gov/news.release/disabl.htm).
Winkleby, Marilyn A., D. E. Jatulis, E. Frank, and S. P. Fortmann. 1992. “Socioeconomic Status and Health: How Education, Income, and Occupation Contribute to Risk Factors for Cardiovascular Disease.” American Journal of Public Health 82:6.
13.4 Comparative Health and Medicine
Anders, George. 1996. Health Against Wealth: HMOs and the Breakdown of Medical Trust. Boston: Houghton Mifflin.
Centers for Disease Control and Prevention. 2014 “Attention Deficit/Hyperactivity Disorder (ADHD) Data and Statistics.” Retrieved October 13, 2014 (http://www.cdc.gov/ncbddd/adhd/data.html)
Docteur, Elizabeth, and Robert A. Berenson. 2009. “How Does the Quality of U.S. Health Care Compare Internationally?” Timely Analysis of Immediate Health Policy Issues 9:1–14.
Kaiser Family Foundation. 2011. “Health Coverage of Children: The Role of Medicaid and CHIP.” Retrieved December 13, 2011 (http://www.kff.org/uninsured/upload/7698-05.pdf).
Kaiser Family Foundation. 2010. “International Health Systems: Canada.” Retrieved December 14, 2011 (http://www.kaiseredu.org/Issue-Modules/International-Health-Systems/Canada.aspx).
Klein, Ezra. 2009. “Health Reform for Beginners: The Difference between Socialized Medicine, Single-Payer Health Care, and What We’ll Be Getting.” The Washington Post, December 14. Retrieved December 15, 2011 (http://www.bloomberg.com/news/2011-12-15/don-t-let-death-panels-kill-a-better-way-to-die-commentary-by-ezra-klein.html).
Kogan, Richard. 2011. “Program Cuts Under a Balanced Budget Amendment: How Severe Might They Be?” Center on Budget and Policy Priorities. Retrieved December 15, 2011 (http://www.cbpp.org/cms/?fa=view&id=3619).
Pear, Robert. 2011. “In Cuts to Health Programs, Experts See Difficult Task in Protecting Patients.” The New York Times, September 20. Retrieved December 13, 2011 (http://www.nytimes.com/2011/09/21/us/politics/wielding-the-ax-on-medicaid-and-medicare-without-wounding-the-patient.html).
Schoen, C., M.M. Doty, R.H. Robertson, and S.R. Collins. 2011. “Affordable Care Act Reforms Could Reduce the Number of Underinsured U.S. Adults by 70 Percent.” Health Affairs 30(9):1762–71. Retrieved December 13, 2011 (http://www.commonwealthfund.org/Publications/In-the-Literature/2011/Sep/Reduce-Uninsured.aspx).
Uchiyma, T., M. Kurosawa, Y. Inaba. 2007. “MMR-Vaccine and Regression in Autism Spectrum Disorders: Negative Results Presented from Japan.” Journal of Autism and Deviant Disorders 37(2):210–7.
U.S. Census. 2011. “Coverage by Type of Health Insurance: 2009 and 2010.” U.S. Census Bureau, Current Population Survey, 2010 and 2011 Annual Social and Economic Supplements. Retrieved December 13, 2011 (http://www.census.gov/hhes/www/hlthins/data/incpovhlth/2010/table10.pdf).
U.S. Census. 2011. “CPS Health Insurance Definitions.” Retrieved December 13, 2011 (http://www.census.gov/hhes/www/hlthins/methodology/definitions/cps.html).
Washington University Center for Health Policy. n.d. “Health Care Access for Medicaid Patients—Physicians and Dentists Interview Study.” Retrieved December 15, 2011 (http://healthpolicy.wustl.edu/Content/HealthCareAccess.html?OpenDocument).
World Health Organization. 2011. “World Health Statistics 2011.” Retrieved December 12, 2011 (http://www.who.int/gho/publications/world_health_statistics/EN_WHS2011_Part1.pdf).
World Health Organization. 2014. “Ebola Virus Disease Fact Sheet, Updated September 2014.” Retrieved October 19, 2014 (http://www.who.int/mediacentre/factsheets/fs103/en/).
13.5 Theoretical Perspectives on Health and Medicine
Conrad, Peter, and Joseph W. Schneider. 1992. Deviance and Medicalization: From Badness to Sickness. Philadelphia, PA: Temple University Press
Parsons, Talcott. 1951. The Social System. Glencoe, IL: Free Press.
Scheff, Thomas. 1963. “The Role of the Mentally Ill and the Dynamics of Mental Disorder.” Sociometry 26:436–453.
